

Clinically-relevant consecutive treatment with isoproterenol and adenosine protects the failing heart against ischaemia and reperfusion
- PMID: 24885907
- PMCID: PMC4045901
- DOI: 10.1186/1479-5876-12-139
Clinically-relevant consecutive treatment with isoproterenol and adenosine protects the failing heart against ischaemia and reperfusion
Abstract
Background: Consecutive treatment of normal heart with a high dose of isoproterenol and adenosine (Iso/Ade treatment), confers strong protection against ischaemia/reperfusion injury. In preparation for translation of this cardioprotective strategy into clinical practice during heart surgery, we further optimised conditions for this intervention using a clinically-relevant dose of Iso and determined its cardioprotective efficacy in hearts isolated from a model of surgically-induced heart failure.
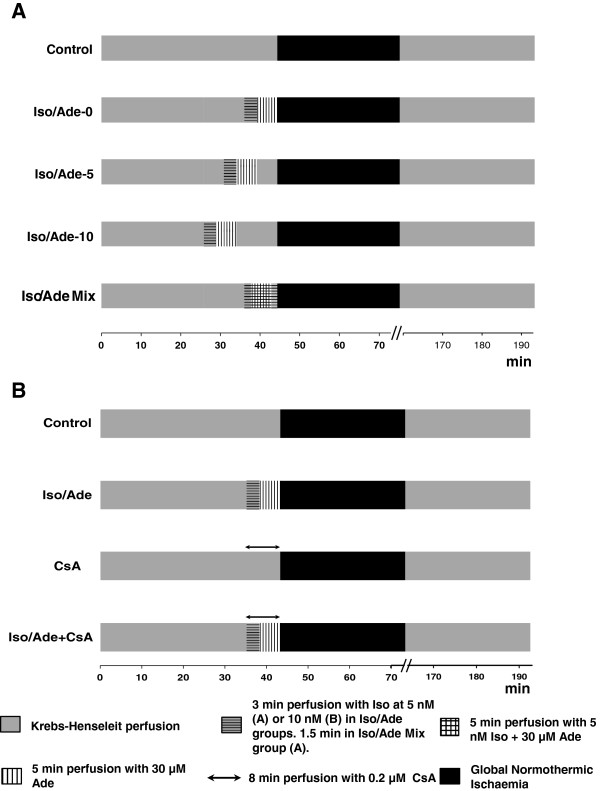
Methods: Isolated Langendorff-perfused rat hearts were treated sequentially with 5 nM Iso and 30 μM Ade followed by different durations of washout prior to 30 min global ischaemia and 2 hrs reperfusion. Reperfusion injury was assessed by measuring haemodynamic function, lactate dehydrogenase (LDH) release and infarct size. Protein kinase C (PKC) activity and glycogen content were measured in hearts after the treatment. In a separate group of hearts, Cyclosporine A (CsA), a mitochondria permeability transition pore (MPTP) inhibitor, was added with Iso/Ade. Failing hearts extracted after 16 weeks of ligation of left coronary artery in 2 months old rats were also subjected to Iso/Ade treatment followed by ischaemia/reperfusion.
Results: Recovery of the rate pressure product (RPP) in Iso/Ade-treated hearts was significantly higher than in controls. Thus in Iso/Ade treated hearts with 5 nM Iso and no washout period, RPP recovery was 76.3±6.9% of initial value vs. 28.5±5.2% in controls. This was associated with a 3 fold reduction in LDH release irrespective to the duration of the washout period. Hearts with no washout of the drugs (Ade) had least infarct size, highest PKC activity and also showed reduced glycogen content. Cardioprotection with CsA was not additive to the effect of Iso/Ade treatment. Iso/Ade treatment conferred significant protection to failing hearts. Thus, RPP recovery in failing hearts subjected to the treatment was 69.0±16.3% while in Control hearts 19.7±4.0%. LDH release in these hearts was also 3 fold lower compared to Control.
Conclusions: Consecutive Iso/Ade treatment of normal heart can be effective at clinically-relevant doses and this effect appears to be mediated by glycogen depletion and inhibition of MPTP. This intervention protects clinically relevant failing heart model making it a promising candidate for clinical use.
Figures






Similar articles
-
Preconditioning or Postconditioning with 8-Br-cAMP-AM Protects the Heart against Regional Ischemia and Reperfusion: A Role for Mitochondrial Permeability Transition.Cells. 2021 May 17;10(5):1223. doi: 10.3390/cells10051223. Cells. 2021. PMID: 34067674 Free PMC article.
-
Consecutive Isoproterenol and Adenosine Treatment Confers Marked Protection against Reperfusion Injury in Adult but Not in Immature Heart: A Role for Glycogen.Int J Mol Sci. 2018 Feb 7;19(2):494. doi: 10.3390/ijms19020494. Int J Mol Sci. 2018. PMID: 29414860 Free PMC article.
-
Consecutive pharmacological activation of PKA and PKC mimics the potent cardioprotection of temperature preconditioning.Cardiovasc Res. 2010 Nov 1;88(2):324-33. doi: 10.1093/cvr/cvq190. Epub 2010 Jun 16. Cardiovasc Res. 2010. PMID: 20558443 Free PMC article.
-
A novel estrogen receptor GPER inhibits mitochondria permeability transition pore opening and protects the heart against ischemia-reperfusion injury.Am J Physiol Heart Circ Physiol. 2010 Jan;298(1):H16-23. doi: 10.1152/ajpheart.00588.2009. Epub 2009 Oct 30. Am J Physiol Heart Circ Physiol. 2010. PMID: 19880667 Free PMC article.
-
Temperature preconditioning of isolated rat hearts--a potent cardioprotective mechanism involving a reduction in oxidative stress and inhibition of the mitochondrial permeability transition pore.J Physiol. 2007 Jun 15;581(Pt 3):1147-61. doi: 10.1113/jphysiol.2007.130369. Epub 2007 Mar 29. J Physiol. 2007. PMID: 17395631 Free PMC article.
Cited by
-
Functional and cardioprotective effects of simultaneous and individual activation of protein kinase A and Epac.Br J Pharmacol. 2017 Mar;174(6):438-453. doi: 10.1111/bph.13709. Epub 2017 Feb 14. Br J Pharmacol. 2017. PMID: 28071786 Free PMC article.
-
Preoperative consecutive treatment with isoprenaline and adenosine is safe and reduces ischaemia-reperfusion injury in a porcine model of cardiac surgery with recent acute myocardial infarction.Eur J Cardiothorac Surg. 2025 May 6;67(5):ezaf120. doi: 10.1093/ejcts/ezaf120. Eur J Cardiothorac Surg. 2025. PMID: 40184215 Free PMC article.
-
Preconditioning or Postconditioning with 8-Br-cAMP-AM Protects the Heart against Regional Ischemia and Reperfusion: A Role for Mitochondrial Permeability Transition.Cells. 2021 May 17;10(5):1223. doi: 10.3390/cells10051223. Cells. 2021. PMID: 34067674 Free PMC article.
-
The role of hexokinase in cardioprotection - mechanism and potential for translation.Br J Pharmacol. 2015 Apr;172(8):2085-100. doi: 10.1111/bph.12899. Epub 2014 Nov 24. Br J Pharmacol. 2015. PMID: 25204670 Free PMC article. Review.
-
Size-Dependent Ability of Liposomes to Accumulate in the Ischemic Myocardium and Protect the Heart.J Cardiovasc Pharmacol. 2018 Sep;72(3):143-152. doi: 10.1097/FJC.0000000000000606. J Cardiovasc Pharmacol. 2018. PMID: 29927783 Free PMC article.
References
-
- Khaliulin I, Clarke SJ, Lin H, Parker JE, Suleiman MS, Halestrap AP. Temperature preconditioning of isolated rat hearts - a potent cardioprotective mechanism involving a reduction in oxidative stress and inhibition of the mitochondrial permeability transition pore. J Physiol. 2007;581:1147–1161. doi: 10.1113/jphysiol.2007.130369. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
