

Towards the clinical implementation of pharmacogenetics in bipolar disorder
- PMID: 24885933
- PMCID: PMC4039055
- DOI: 10.1186/1741-7015-12-90
Towards the clinical implementation of pharmacogenetics in bipolar disorder
Abstract
Background: Bipolar disorder (BD) is a psychiatric illness defined by pathological alterations between the mood states of mania and depression, causing disability, imposing healthcare costs and elevating the risk of suicide. Although effective treatments for BD exist, variability in outcomes leads to a large number of treatment failures, typically followed by a trial and error process of medication switches that can take years. Pharmacogenetic testing (PGT), by tailoring drug choice to an individual, may personalize and expedite treatment so as to identify more rapidly medications well suited to individual BD patients.
Discussion: A number of associations have been made in BD between medication response phenotypes and specific genetic markers. However, to date clinical adoption of PGT has been limited, often citing questions that must be answered before it can be widely utilized. These include: What are the requirements of supporting evidence? How large is a clinically relevant effect? What degree of specificity and sensitivity are required? Does a given marker influence decision making and have clinical utility? In many cases, the answers to these questions remain unknown, and ultimately, the question of whether PGT is valid and useful must be determined empirically. Towards this aim, we have reviewed the literature and selected drug-genotype associations with the strongest evidence for utility in BD.
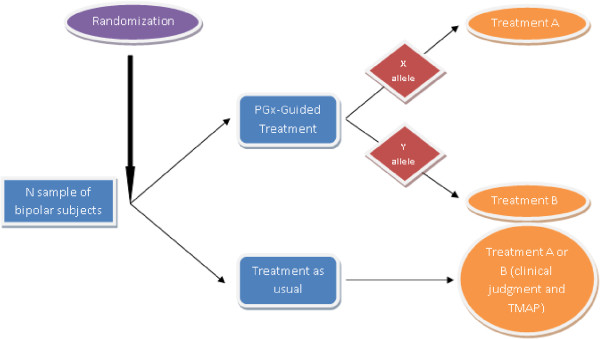
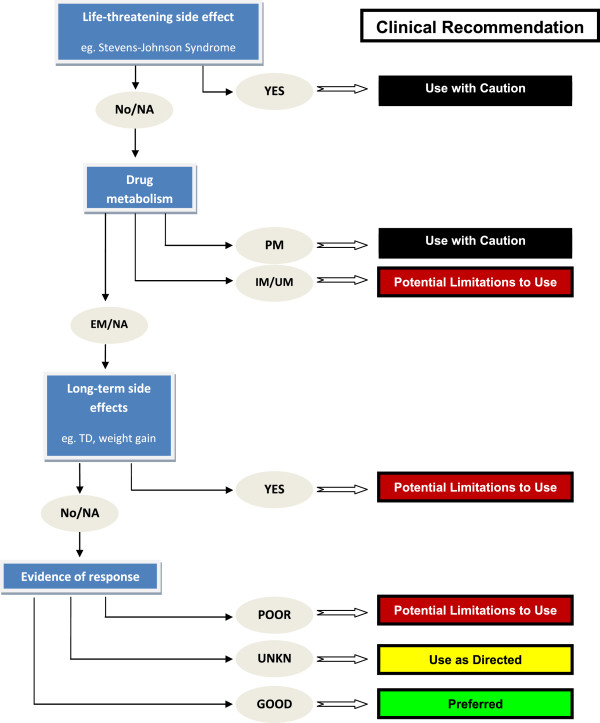
Summary: Based upon these findings, we propose a preliminary panel for use in PGT, and a method by which the results of a PGT panel can be integrated for clinical interpretation. Finally, we argue that based on the sufficiency of accumulated evidence, PGT implementation studies are now warranted. We propose and discuss the design for a randomized clinical trial to test the use of PGT in the treatment of BD.
Figures
References
-
- Yatham LN, Kennedy SH, Schaffer A, Parikh SV, Beaulieu S, O’Donovan C, MacQueen G, McIntyre RS, Sharma V, Ravindran A, Young LT, Young AH, Alda M, Milev R, Vieta E, Calabrese JR, Berk M, Ha K, Kapczinski F. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) collaborative update of CANMAT guidelines for the management of patients with bipolar disorder: update 2009. Bipolar Disord. 2009;11:225–255. doi: 10.1111/j.1399-5618.2009.00672.x. - DOI - PubMed
-
- Suppes T, Dennehy EB, Hirschfeld RM, Altshuler LL, Bowden CL, Calabrese JR, Crismon ML, Ketter TA, Sachs GS, Swann AC. The Texas implementation of medication algorithms: update to the algorithms for treatment of bipolar I disorder. J Clin Psychiatry. 2005;66:870–886. doi: 10.4088/JCP.v66n0710. - DOI - PubMed
-
- Hirschfeld RM, Lewis L, Vornik LA. Perceptions and impact of bipolar disorder: how far have we really come? Results of the national depressive and manic-depressive association 2000 survey of individuals with bipolar disorder. J Clin Psychiatry. 2003;64:161–174. doi: 10.4088/JCP.v64n0209. - DOI - PubMed
