

Olanzapine is superior to lamotrigine in the prevention of bipolar depression: a naturalistic observational study
- PMID: 24885966
- PMCID: PMC4035822
- DOI: 10.1186/1471-244X-14-145
Olanzapine is superior to lamotrigine in the prevention of bipolar depression: a naturalistic observational study
Abstract
Background: Bipolar disorder is a highly recurrent disease and has great impact on the function of patients. Depressive symptoms consist of more than 50% of life time during the illness and may lead to self harm or suicidal behaviors. Little is known about the antidepressant effects of olanzapine, an atypical antipsychotic, as monotherapy despite its indication for preventing manic episodes. In contrast, lamotrigine, a mood stabilizer, has been proven to be effective in preventing depression in patients with bipolar disorder. However, no studies have compared the efficacy between lamotrigine and olanzapine in the maintenance treatment of bipolar disorder. This enriched naturalistic study was implemented to assess the effectiveness of olanzapine and lamotrigine as monotherapy in the prevention of recurrence of bipolar disorder.
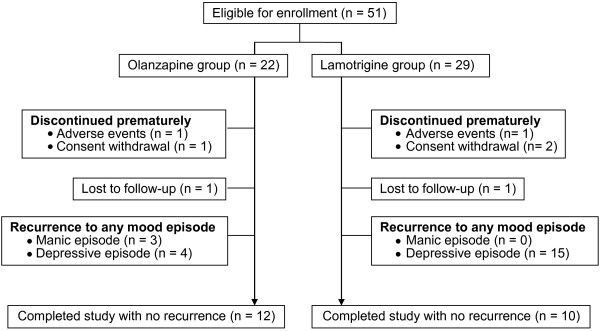
Methods: Patients with bipolar disorder in a euthymic state (Young's Mania Rating Scale (YMRS) score <12, and 21-item Hamilton Depression Rating Scale (HAM-D) score <7) for at least two months, having already received either olanzapine or lamotrigine as the maintenance treatment were recruited. The patients maintained with olanzapine (n = 22) were applied to olanzapine group whereas those maintained with lamotrigine (n = 29) were applied to lamotrigine group. They were followed up for 12 months. Differences in the efficacy between olanzapine and lamotrigine in recurrence prevention were analyzed. The Kaplan-Meier method was used to generate time-to-recurrence curves, and differences between the two groups were compared using the log-rank test.
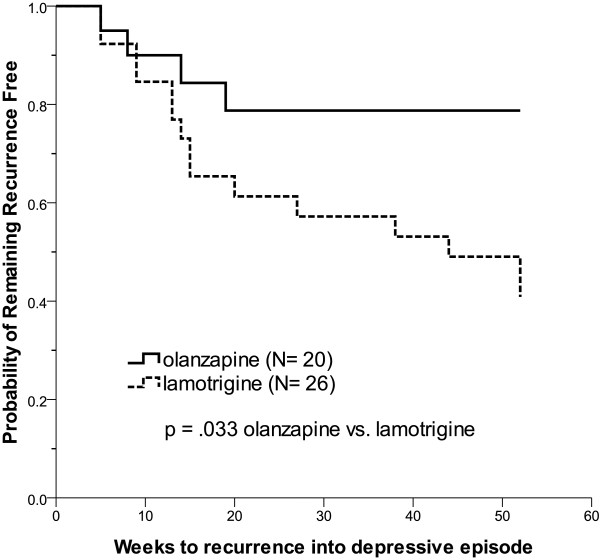
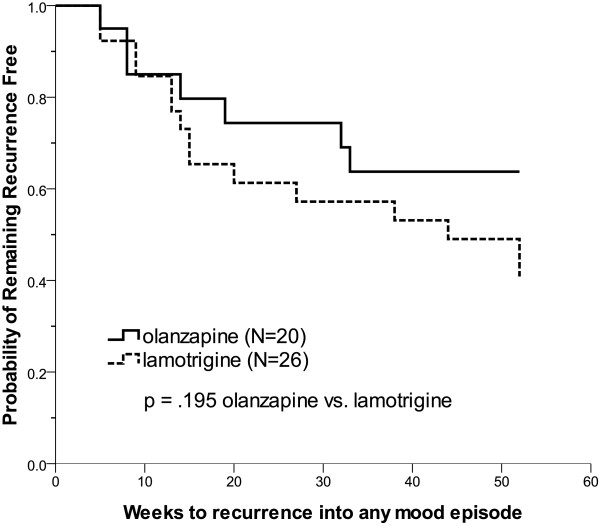
Results: Olanzapine had a significantly lower recurrence rate of depressive episodes than lamotrigine (20.0% vs. 57.7%, χ2 = 6.62, p = .010). However, olanzapine and lamotrigine had similar mania (15.0% vs. 0%, χ2 = 4.17, p = .075, Fisher's exact test) and any mood episode (35.0% vs. 57.7%, χ2 = 2.33, p = .127) recurrence rates. Olanzapine was significantly superior to lamotrigine in the time to recurrence of depressive episodes (χ2 = 4.55, df = 1, p = .033), but there was no difference in the time to recurrence of any mood episode (χ2 = 1.68, df = 1, p = .195).
Conclusions: This prospective naturalistic study suggests that olanzapine is more effective than lamotrigine in the prevention of depressive episodes in patients with bipolar disorder. Future large-scale randomized studies are warranted to validate our results.
Trial registration: ClinicalTrials.gov ID NCT01864551.
Figures
Similar articles
-
[Antipsychotics in bipolar disorders].Encephale. 2004 Sep-Oct;30(5):417-24. doi: 10.1016/s0013-7006(04)95456-5. Encephale. 2004. PMID: 15627046 Review. French.
-
The cost-effectiveness of lamotrigine in the maintenance treatment of adults with bipolar I disorder.J Manag Care Pharm. 2006 May;12(4):322-30. doi: 10.18553/jmcp.2006.12.4.322. J Manag Care Pharm. 2006. PMID: 16792438 Free PMC article.
-
Olanzapine or lamotrigine addition to lithium in remitted bipolar disorder patients with anxiety disorder comorbidity: a randomized, single-blind, pilot study.J Clin Psychiatry. 2008 Apr;69(4):609-16. doi: 10.4088/jcp.v69n0413. J Clin Psychiatry. 2008. PMID: 18294024 Clinical Trial.
-
Lamotrigine compared to placebo and other agents with antidepressant activity in patients with unipolar and bipolar depression: a comprehensive meta-analysis of efficacy and safety outcomes in short-term trials.CNS Spectr. 2016 Oct;21(5):403-418. doi: 10.1017/S1092852916000523. CNS Spectr. 2016. PMID: 27686028
-
Newer treatment studies for bipolar depression.Bipolar Disord. 2005;7 Suppl 5:13-23. doi: 10.1111/j.1399-5618.2005.00250.x. Bipolar Disord. 2005. PMID: 16225556 Review.
Cited by
-
Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder.Bipolar Disord. 2018 Mar;20(2):97-170. doi: 10.1111/bdi.12609. Epub 2018 Mar 14. Bipolar Disord. 2018. PMID: 29536616 Free PMC article.
-
Efficacy and safety of lamotrigine in the treatment of bipolar disorder across the lifespan: a systematic review.Ther Adv Psychopharmacol. 2021 Oct 8;11:20451253211045870. doi: 10.1177/20451253211045870. eCollection 2021. Ther Adv Psychopharmacol. 2021. PMID: 34646439 Free PMC article. Review.
References
-
- Gitlin MJ, Swendsen J, Heller TL, Hammen C. Relapse and impairment in bipolar disorder. Am J Psychiatry. 1995;152(11):1635–40. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
