

Does induction of labor for constitutionally large-for-gestational-age fetuses identified in utero reduce maternal morbidity?
- PMID: 24885981
- PMCID: PMC4012520
- DOI: 10.1186/1471-2393-14-156
Does induction of labor for constitutionally large-for-gestational-age fetuses identified in utero reduce maternal morbidity?
Abstract
Background: The number of infants with a birth weight > 97th percentile for gestational age has increased over the years. Although some studies have examined the interest of inducing labor for fetuses with macrosomia suspected in utero, only a few have analyzed this suspected macrosomia according to estimated weight at each gestational age. Most studies have focused principally on neonatal rather than on maternal (and still less on perineal) outcomes. The principal aim of this study was to assess whether a policy of induction of labor for women with a constitutionally large-for-gestational-age fetus might reduce the occurrence of severe perineal tears; the secondary aims of this work were to assess whether this policy would reduce either recourse to cesarean delivery during labor or neonatal complications.
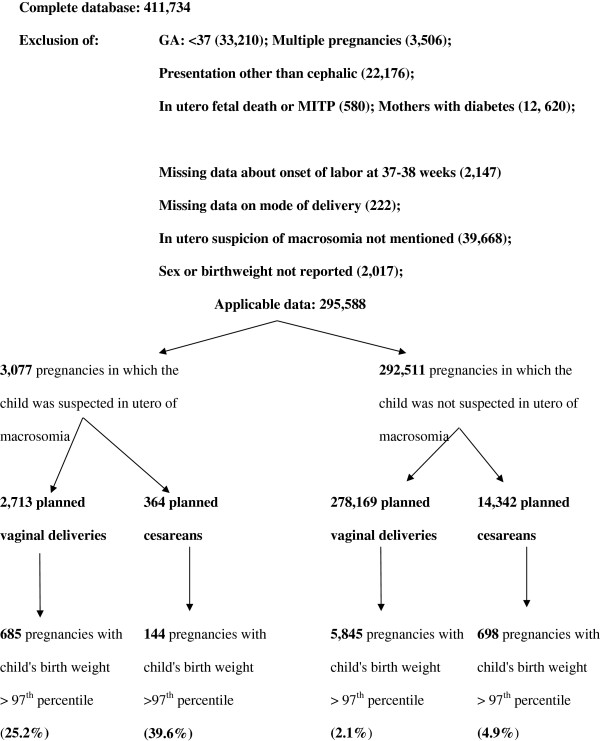
Methods: This historical cohort study (n = 3077) analyzed records from a French perinatal database. Women without diabetes and with a cephalic singleton term pregnancy were eligible for the study. We excluded medically indicated terminations of pregnancy and in utero fetal deaths. Among the pregnancies with fetuses suspected, before birth, of being large-for-gestational-age, we compared those for whom labor was induced from ≥ 37 weeks to ≤ 38 weeks+ 6 days (n = 199) to those with expectant obstetrical management (n = 2878). In this intention-to-treat analysis, results were expressed as crude and adjusted relative risks.
Results: The mean birth weight was 4012 g ± 421 g. The rate of perineal lesions did not differ between the two groups in either primiparas (aRR: 1.06; 95% CI: 0.86-1.31) or multiparas (aRR: 0.94; 95% CI: 0.84-1.05). Similarly, neither the cesarean rate (aRR: 1.11; 95% CI: 0.82-1.50) nor the risks of resuscitation in the delivery room or of death in the delivery room or in the immediate postpartum or of neonatal transfer to the NICU (aRR = 0.94; 95% CI: 0.59-1.50) differed between the two groups.
Conclusions: A policy of induction of labor for women with a constitutionally large-for-gestational-age fetus among women without diabetes does not reduce maternal morbidity.
Figures
Similar articles
-
Is prenatal identification of fetal macrosomia useful?Eur J Obstet Gynecol Reprod Biol. 2012 Apr;161(2):170-6. doi: 10.1016/j.ejogrb.2012.01.010. Epub 2012 Feb 10. Eur J Obstet Gynecol Reprod Biol. 2012. PMID: 22326615
-
Maternal and newborn outcomes with elective induction of labor at term.Am J Obstet Gynecol. 2019 Mar;220(3):273.e1-273.e11. doi: 10.1016/j.ajog.2019.01.223. Epub 2019 Feb 17. Am J Obstet Gynecol. 2019. PMID: 30716284
-
Induction of labour at or beyond 37 weeks' gestation.Cochrane Database Syst Rev. 2020 Jul 15;7(7):CD004945. doi: 10.1002/14651858.CD004945.pub5. Cochrane Database Syst Rev. 2020. PMID: 32666584 Free PMC article.
-
[In case of fetal macrosomia, the best strategy is the induction of labor at 38 weeks of gestation].J Gynecol Obstet Biol Reprod (Paris). 2016 Nov;45(9):1037-1044. doi: 10.1016/j.jgyn.2016.09.001. Epub 2016 Oct 19. J Gynecol Obstet Biol Reprod (Paris). 2016. PMID: 27771202 Review. French.
-
Elective induction of labor at term compared with expectant management: maternal and neonatal outcomes.Obstet Gynecol. 2013 Oct;122(4):761-769. doi: 10.1097/AOG.0b013e3182a6a4d0. Obstet Gynecol. 2013. PMID: 24084532 Free PMC article.
Cited by
-
Validating machine learning models for the prediction of labour induction intervention using routine data: a registry-based retrospective cohort study at a tertiary hospital in northern Tanzania.BMJ Open. 2021 Dec 2;11(12):e051925. doi: 10.1136/bmjopen-2021-051925. BMJ Open. 2021. PMID: 34857568 Free PMC article.
References
-
- Association des Utilisateurs de Dossiers Informatisés en Pédiatrie, Obstétrique et Gynécologie. Database access. [ http://www.audipog.net/interro-choix.php] - PubMed
-
- Collège National des Gynécologues et Obstétriciens Français. French episiotomy guideline 2006. [ http://www.cngof.asso.fr/D_PAGES/PURPC_14.HTM]
-
- De Leeuw JW, Struijk PC, Vierhout ME, Walleburg HCS. Risk factors for third degree perineal ruptures during deliver. Bri J Obstet Gynaecol. 2001;108:383–387. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
