

Anaesthesia in patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy: retrospective analysis of a single centre three-year experience
- PMID: 24886171
- PMCID: PMC4113247
- DOI: 10.1186/1477-7819-12-136
Anaesthesia in patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy: retrospective analysis of a single centre three-year experience
Abstract
Background: Cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy (CRS/HIPEC) is a treatment option for selected patients with peritoneal carcinomatosis. There are limited data available on anaesthesia management and its impact on patients' outcome. Our aim was to retrospectively analyze and evaluate perioperative management and the clinical course of patients undergoing CRS/HIPEC within a three-year period.
Methods: After ethic committee approval, patient charts were retrospectively reviewed for patient characteristics, interventions, perioperative management, postoperative course, and complications. Analysis was intervention based. Data are presented as median (range).
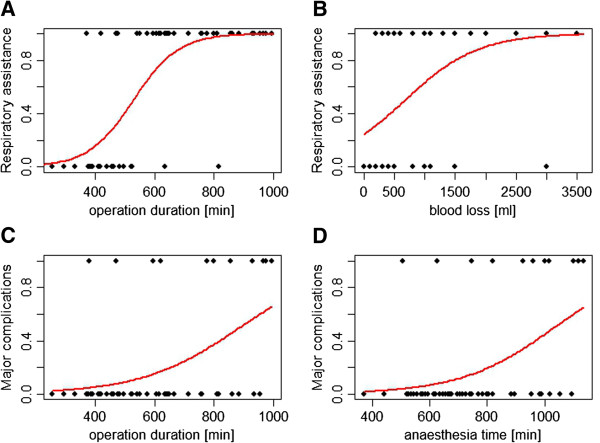
Results: Between 2009 and 2011, 54 consecutive patients underwent 57 interventions; median anaesthesia time was 715 (range 370 to 1135) minutes. HIPEC induced hyperthermia with an overall median peak temperature of 38.1 (35.7-40.2)°C with active cooling. Bleeding, expressed as median blood loss was 0.8 (0 to 6) litre and large fluid shifts occurred, requiring a total fluid input of 8.4 (4.2 to 29.4) litres per patient. Postoperative renal function was dependent on preoperative function and the type of fluids used. Administration of hydroxyethyl starch colloid solution had a significant negative impact on renal function, especially in younger patients. Major complications occurred after 12 procedures leading to death in 2 patients. Procedure time and need for blood transfusion were associated with a significantly higher risk for major complications.
Conclusions: Cytoreductive surgery with HIPEC is a high-risk surgical procedure associated with major hemodynamic and metabolic changes. As well as primary disease and complexity of surgery, we have shown that anaesthesia management, the type and amount of fluids used, and blood transfusions may also have a significant effect on patients' outcome.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
