

Assessment of atropine-sufentanil-atracurium anaesthesia for endotracheal intubation: an observational study in very premature infants
- PMID: 24886350
- PMCID: PMC4028002
- DOI: 10.1186/1471-2431-14-120
Assessment of atropine-sufentanil-atracurium anaesthesia for endotracheal intubation: an observational study in very premature infants
Abstract
Background: Premedication before neonatal intubation is heterogeneous and contentious. The combination of a short acting, rapid onset opioid with a muscle relaxant is considered suitable by many experts. The purpose of this study was to describe the tolerance and conditions of intubation following anaesthesia with atropine, sufentanil and atracurium in very premature infants.
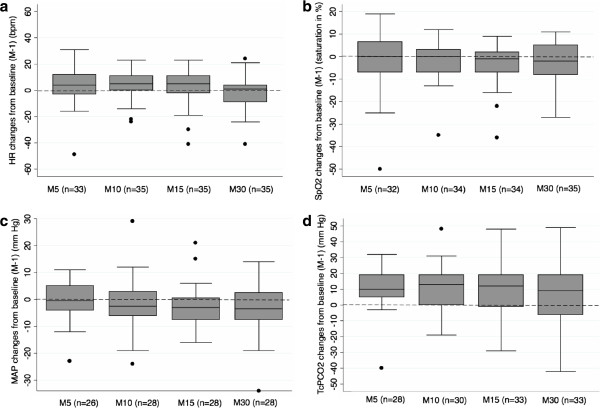
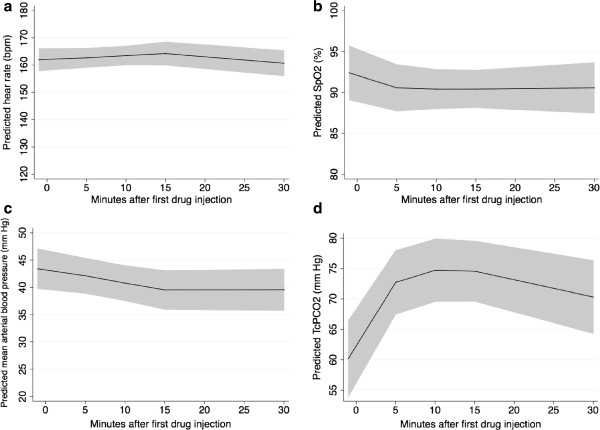
Methods: Monocentric, prospective observational study in premature infants born before 32 weeks of gestational age, hospitalised in the NICU and requiring semi-urgent or elective intubation. Intubation conditions, heart rate, pulse oxymetry (SpO2), arterial blood pressure and transcutaneous PCO2 (TcPCO2) were collected in real time during 30 minutes following the first drug injection. Repeated physiological measurements were analysed using mixed linear models.
Results: Thirty five intubations were performed in 24 infants with a median post conceptional age of 27.6 weeks and a median weight of 850 g at the time of intubation. The first attempt was successful in 74% and was similar for junior (75%) and senior (74%) operators. The operator rated conditions as "excellent" or "good" in 94% of intubations. A persistent increase in TcPCO2 as compared to baseline was observed whereas other vital parameters showed no significant variations 5, 10, 15 and 30 minutes after the first drug injection. Eighteen (51%) desaturations (SpO2 less than or equal to 80% for more than 60 seconds) and 2 (6%) bradycardia (heart rate less than 100 bpm for more than 60 seconds) were observed.
Conclusion: This drug combination offers satisfactory success rate for first attempt and intubation conditions for the operator without any significant change in heart rate and blood pressure for the patient. However it is associated with frequent desaturations and a possible persistent hypercapnia. SpO2 and PCO2 can be significantly modified during neonatal intubation and should be cautiously followed in this high-risk population.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
