

Sublobectomy versus lobectomy for stage IA (T1a) non-small-cell lung cancer: a meta-analysis study
- PMID: 24886396
- PMCID: PMC4029973
- DOI: 10.1186/1477-7819-12-138
Sublobectomy versus lobectomy for stage IA (T1a) non-small-cell lung cancer: a meta-analysis study
Abstract
Background: Although lobectomy is considered the standard surgical treatment for the majority of patients with non-small-cell lung cancer (NSCLC), the operation project for patients with stage IA NSCLC (T1a, tumor diameter≤2 cm) remains controversial. Sublobectomy is appropriate only in certain patients as many doctors consider it to be overtreatment. We evaluated the five-year overall survival rate of sublobectomy and lobectomy for stage IA NSCLC (T1a, tumor diameter≤2 cm) through a meta-analysis.
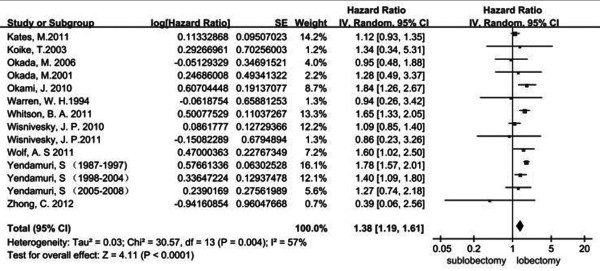
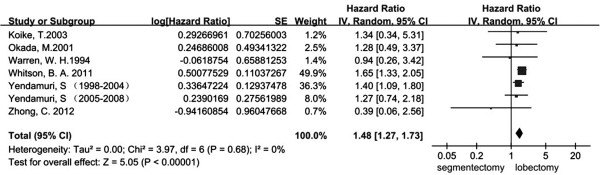
Methods: The five-year overall survival rate (OS) of stage IA (T1a) NSCLC after sublobectomy (including wedge resection and segmentectomy) and lobectomy were compared. We also compared the OS of stage IA (T1a) NSCLC after segmentectomy and lobectomy. The log (hazard ratio, ln (HR)) and its standard error (SE) were used as the outcome measure for data combining.
Results: There were 12 eligible studies published between 1994 and 2013 in which the total number of participants was 18,720. When compared to lobectomy, there was a statistically significant difference of sublobectomy on OS of stage IA (T1a) NSCLC patients (HR 1.38; 95% confidence interval (95% CI), 1.19 to 1.61; P<0.0001). For the comparison between segmentectomy and lobectomy, there was also a statistically significant difference of segmentectomy alone on OS of stage IA (T1a) NSCLC patients (HR 1.48; 95% CI: 1.27 to 1.73; P<0.00001) CONCLUSIONS: We have concluded that in stage IA (T1a) patients sublobectomy, including segmentectomy and wedge resection, causes a lower survival rate than lobectomy.
Figures
References
-
- El-Sherif A, Gooding WE, Santos R, Pettiford B, Ferson PF, Fernando HC, Urda SJ, Luketich JD, Landreneau RJ. Outcomes of sublobar resection versus lobectomy for stage I non–small cell lung cancer: a 13-year analysis. Ann Thorac Surg. 2006;82:408–416. doi: 10.1016/j.athoracsur.2006.02.029. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
