

Analyzing spatial clustering and the spatiotemporal nature and trends of HIV/AIDS prevalence using GIS: the case of Malawi, 1994-2010
- PMID: 24886573
- PMCID: PMC4057596
- DOI: 10.1186/1471-2334-14-285
Analyzing spatial clustering and the spatiotemporal nature and trends of HIV/AIDS prevalence using GIS: the case of Malawi, 1994-2010
Abstract
Background: Although local spatiotemporal analysis can improve understanding of geographic variation of the HIV epidemic, its drivers, and the search for targeted interventions, it is limited in sub-Saharan Africa. Despite recent declines, Malawi's estimated 10.0% HIV prevalence (2011) remained among the highest globally. Using data on pregnant women in Malawi, this study 1) examines spatiotemporal trends in HIV prevalence 1994-2010, and 2) for 2010, identifies and maps the spatial variation/clustering of factors associated with HIV prevalence at district level.
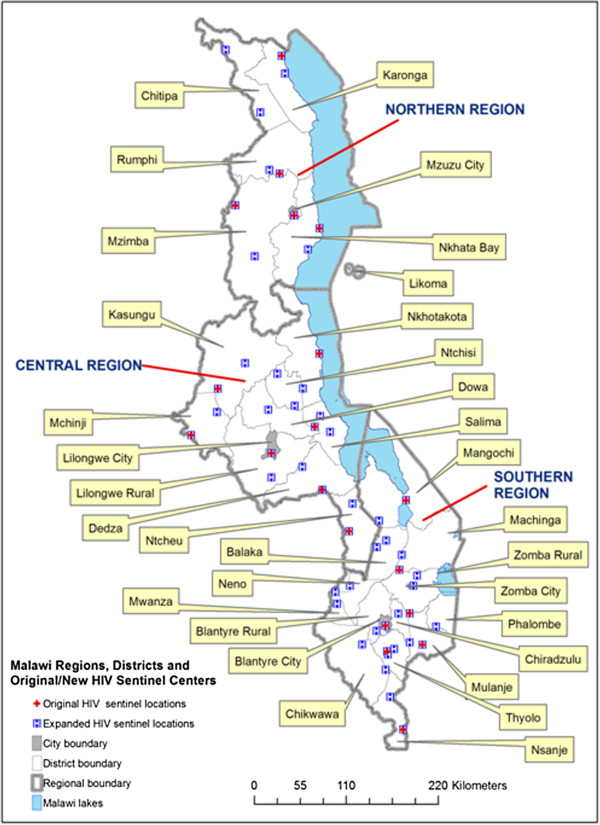
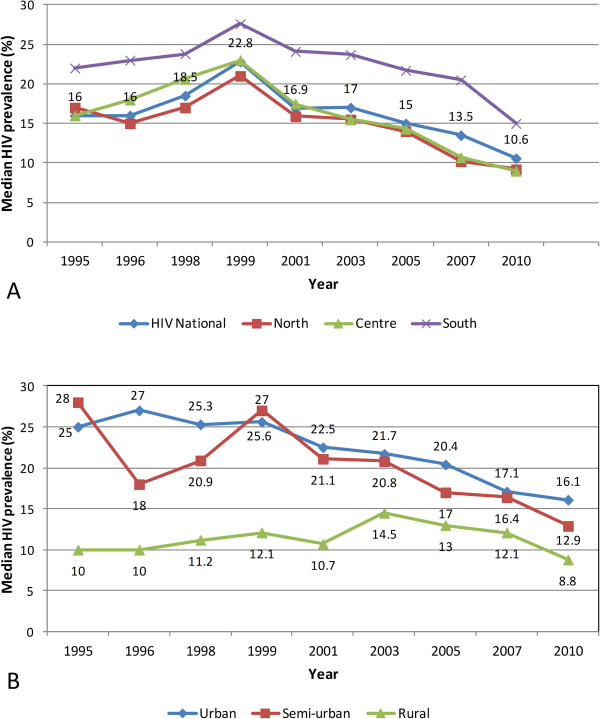
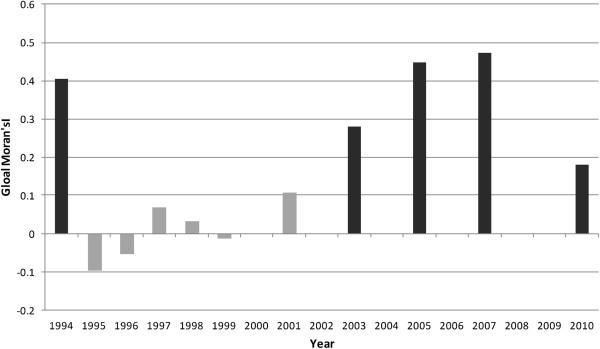
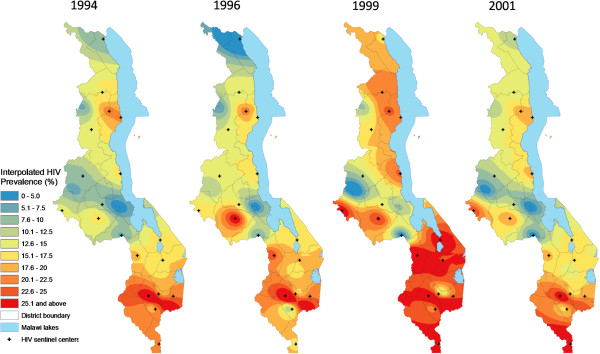
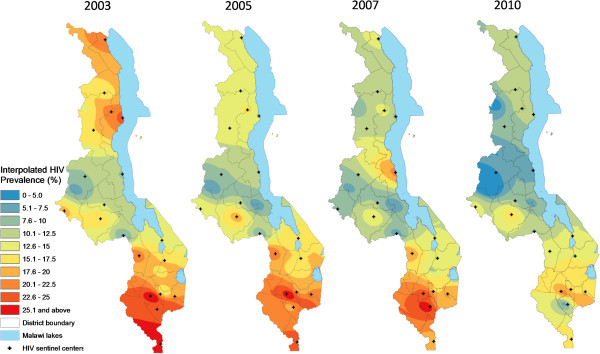
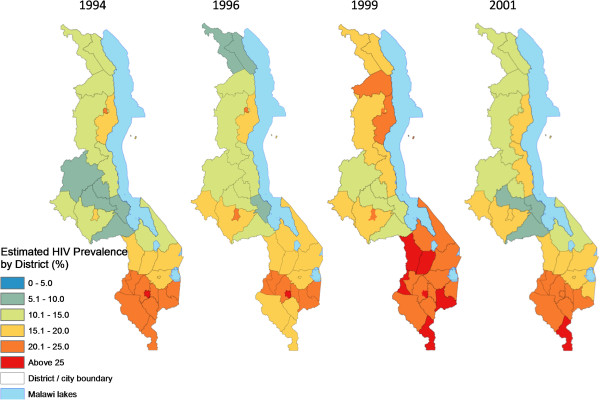
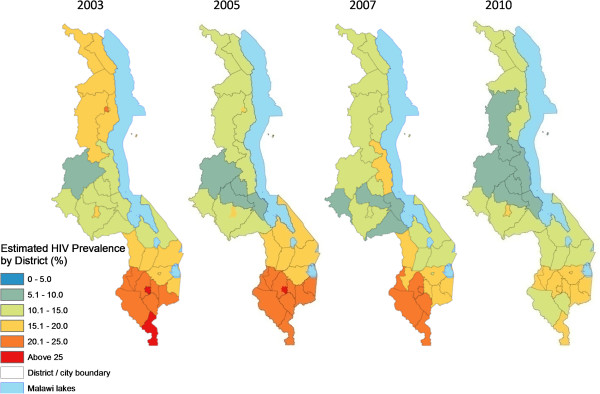
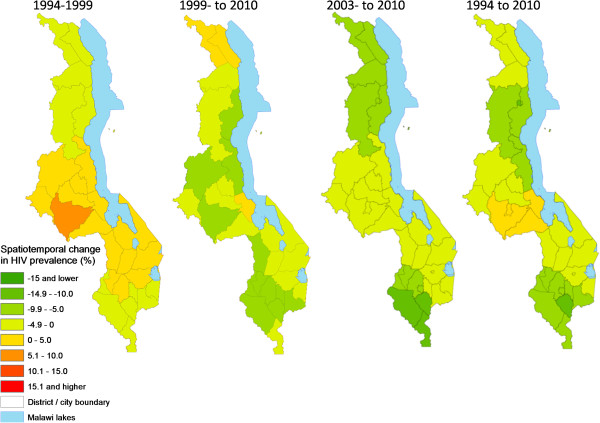
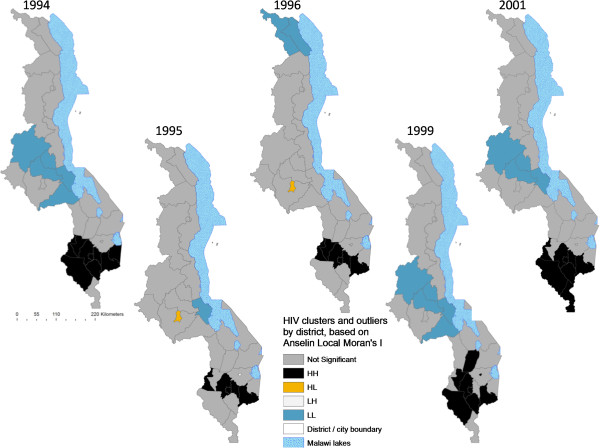
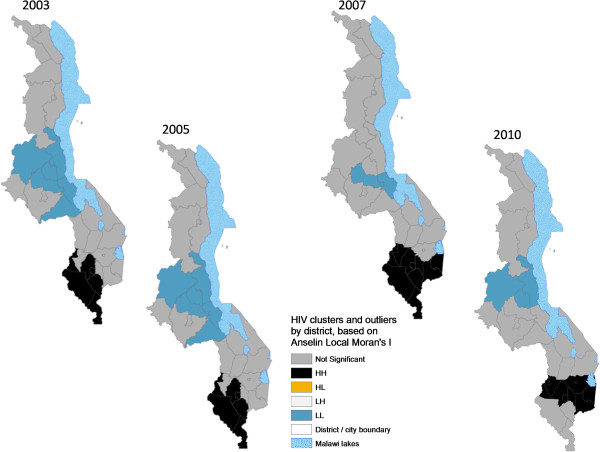
Methods: Inverse distance weighting was used within ArcGIS Geographic Information Systems (GIS) software to generate continuous surfaces of HIV prevalence from point data (1994, 1996, 1999, 2001, 2003, 2005, 2007, and 2010) obtained from surveillance antenatal clinics. From the surfaces prevalence estimates were extracted at district level and the results mapped nationally. Spatial dependency (autocorrelation) and clustering of HIV prevalence were also analyzed. Correlation and multiple regression analyses were used to identify factors associated with HIV prevalence for 2010 and their spatial variation/clustering mapped and compared to HIV clustering.
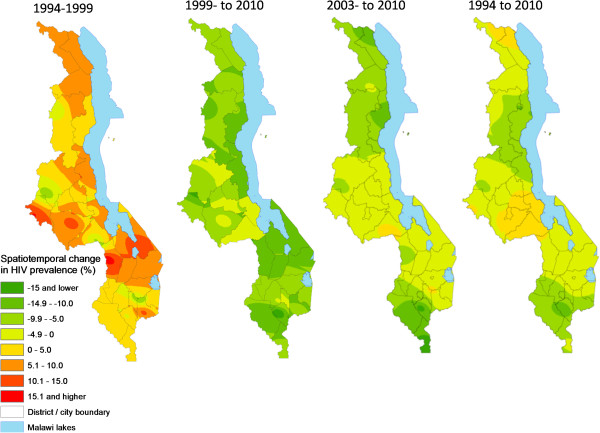
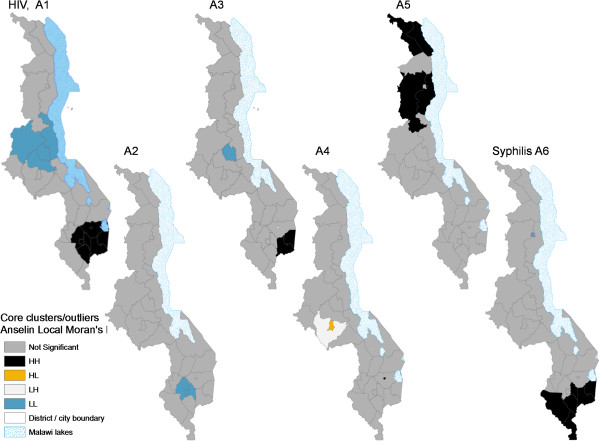
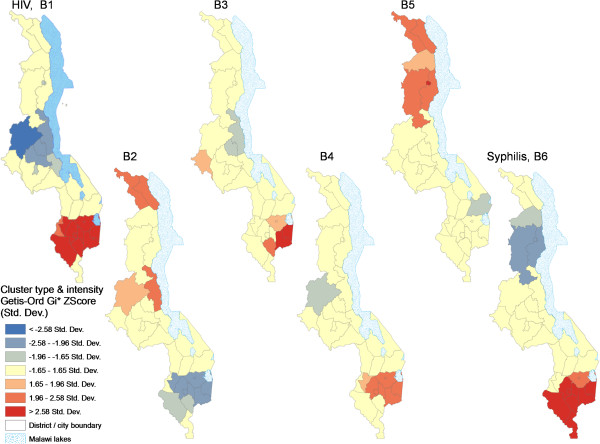
Results: Analysis revealed wide spatial variation in HIV prevalence at regional, urban/rural, district and sub-district levels. However, prevalence was spatially leveling out within and across 'sub-epidemics' while declining significantly after 1999. Prevalence exhibited statistically significant spatial dependence nationally following initial (1995-1999) localized, patchy low/high patterns as the epidemic spread rapidly. Locally, HIV "hotspots" clustered among eleven southern districts/cities while a "coldspot" captured configurations of six central region districts. Preliminary multiple regression of 2010 HIV prevalence produced a model with four significant explanatory factors (adjusted R2 = 0.688): mean distance to main roads, mean travel time to nearest transport, percentage that had taken an HIV test ever, and percentage attaining a senior primary education. Spatial clustering linked some factors to particular subsets of high HIV-prevalence districts.
Conclusions: Spatial analysis enhanced understanding of local spatiotemporal variation in HIV prevalence, possible underlying factors, and potential for differentiated spatial targeting of interventions. Findings suggest that intervention strategies should also emphasize improved access to health/HIV services, basic education, and syphilis management, particularly in rural hotspot districts, as further research is done on drivers at finer scale.
Figures
References
-
- Kalipeni E, Zulu L. Using GIS to model and forecast HIV/AIDS rates in Africa, 1986–2010. Prof Geogr. 2008;14:33–53. doi: 10.1080/00330120701724061. - DOI
-
- Mayer JD. The geographical understanding of HIV/AIDS in sub-Saharan Africa. NorskGeografiskTidsskrift - Norwegian J Geogr. 2005;14:6–13.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
