

Modelling the impact of ivermectin on River Blindness and its burden of morbidity and mortality in African Savannah: EpiOncho projections
- PMID: 24886747
- PMCID: PMC4037555
- DOI: 10.1186/1756-3305-7-241
Modelling the impact of ivermectin on River Blindness and its burden of morbidity and mortality in African Savannah: EpiOncho projections
Abstract
Background: The African Programme for Onchocerciasis Control (APOC) has refocused its goals on the elimination of infection where possible, seemingly achievable by 15-17 years of annual mass distribution of ivermectin in some African foci. Previously, APOC had focused on the elimination of onchocerciasis as a public health problem. Timeframes have been set by the World Health Organization, the London Declaration on Neglected Tropical Diseases and the World Bank to achieve these goals by 2020-2025.
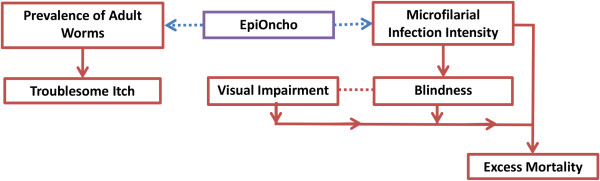
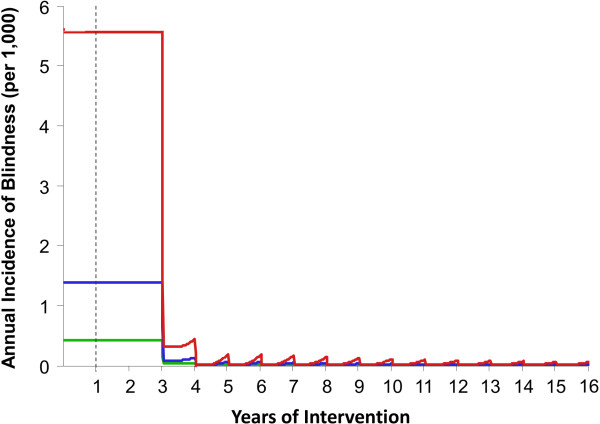
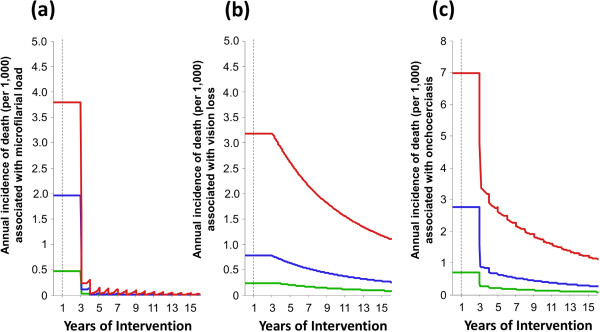
Methods: A novel mathematical model of the dynamics of onchocercal disease is presented which links documented associations between Onchocerca volvulus infection and the prevalence and incidence of morbidity and mortality to model outputs from our host age- and sex-structured onchocerciasis transmission framework (EpiOncho). The model is calibrated for African savannah settings, and used to assess the impact of long-term annual mass administration of ivermectin on infection and ocular and skin disease and to explore how this depends on epidemiological and programmatic variables.
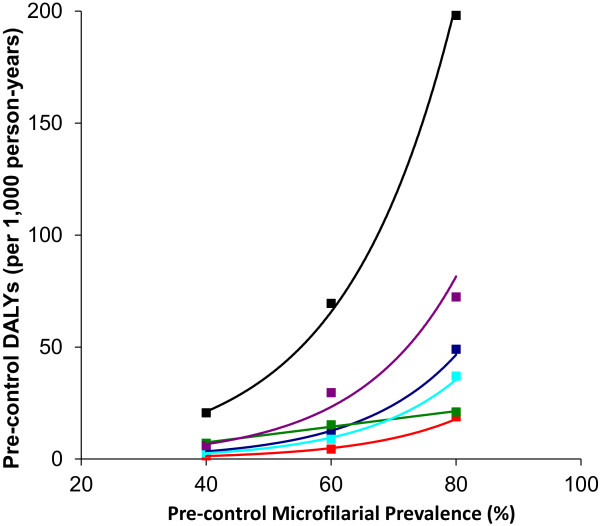
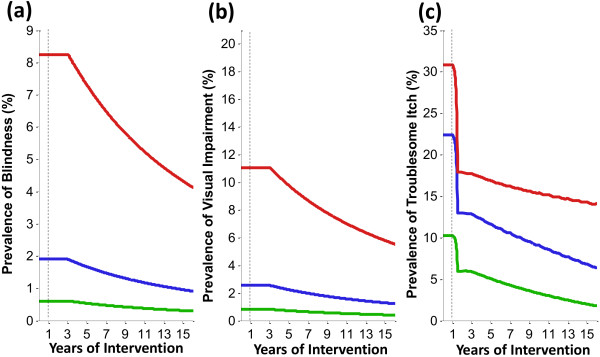
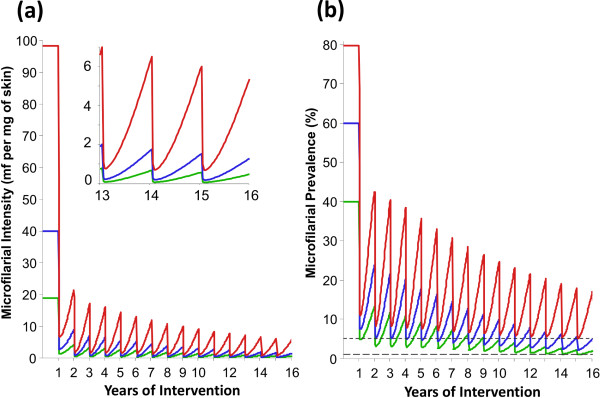
Results: Current onchocerciasis disease projections, which do not account for excess mortality of sighted individuals with heavy microfilarial loads, underestimate disease burden. Long-term annual ivermectin treatment is highly effective at reducing both the morbidity and mortality associated with onchocerciasis, and this result is not greatly influenced by treatment coverage and compliance. By contrast, impact on microfilarial prevalence and intensity is highly dependent on baseline endemicity, treatment coverage and systematic non-compliance.
Conclusions: The goals of eliminating morbidity and infection with ivermectin alone are distinctly influenced by epidemiological and programmatic factors. Whilst the former goal is most certainly achievable, reaching the latter will strongly depend on initial endemicity (the higher the endemicity, the greater the magnitude of inter-treatment transmission), advising caution when generalising the applicability of successful elimination outcomes to other areas. The proportion of systematic non-compliers will become far more influential in terms of overall success in achieving elimination goals.
Figures
Similar articles
-
Reaching the london declaration on neglected tropical diseases goals for onchocerciasis: an economic evaluation of increasing the frequency of ivermectin treatment in Africa.Clin Infect Dis. 2014 Oct;59(7):923-32. doi: 10.1093/cid/ciu467. Epub 2014 Jun 18. Clin Infect Dis. 2014. PMID: 24944228 Free PMC article.
-
Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal.Epidemics. 2017 Mar;18:4-15. doi: 10.1016/j.epidem.2017.02.005. Epidemics. 2017. PMID: 28279455 Free PMC article.
-
The potential impact of moxidectin on onchocerciasis elimination in Africa: an economic evaluation based on the Phase II clinical trial data.Parasit Vectors. 2015 Mar 19;8:167. doi: 10.1186/s13071-015-0779-4. Parasit Vectors. 2015. PMID: 25889256 Free PMC article.
-
River Blindness: Mathematical Models for Control and Elimination.Adv Parasitol. 2016;94:247-341. doi: 10.1016/bs.apar.2016.08.003. Epub 2016 Oct 7. Adv Parasitol. 2016. PMID: 27756456 Review.
-
Onchocercal eye disease and the impact of Mectizan treatment.Ann Trop Med Parasitol. 1998 Apr;92 Suppl 1:S11-22. doi: 10.1080/00034989859519. Ann Trop Med Parasitol. 1998. PMID: 9861263 Review.
Cited by
-
Factors Associated with Ivermectin Non-Compliance and Its Potential Role in Sustaining Onchocerca volvulus Transmission in the West Region of Cameroon.PLoS Negl Trop Dis. 2016 Aug 16;10(8):e0004905. doi: 10.1371/journal.pntd.0004905. eCollection 2016 Aug. PLoS Negl Trop Dis. 2016. PMID: 27529622 Free PMC article.
-
Detection of Onchocerca volvulus in Skin Snips by Microscopy and Real-Time Polymerase Chain Reaction: Implications for Monitoring and Evaluation Activities.Am J Trop Med Hyg. 2016 Apr;94(4):906-11. doi: 10.4269/ajtmh.15-0695. Epub 2016 Feb 15. Am J Trop Med Hyg. 2016. PMID: 26880774 Free PMC article.
-
Development of a High-Throughput Cytometric Screen to Identify Anti- Wolbachia Compounds: The Power of Public-Private Partnership.SLAS Discov. 2019 Jun;24(5):537-547. doi: 10.1177/2472555219838341. Epub 2019 Apr 8. SLAS Discov. 2019. PMID: 30958712 Free PMC article.
-
Status of parasitological indicators and morbidity burden of onchocerciasis after years of successive implementation of mass distribution of ivermectin in selected communities of Yeki and Asosa districts, Ethiopia.BMC Public Health. 2020 Aug 12;20(1):1233. doi: 10.1186/s12889-020-09344-7. BMC Public Health. 2020. PMID: 32787813 Free PMC article.
-
Onchocerciasis is not a major cause of blindness in two endemic villages in Sierra Leone.BMC Res Notes. 2025 Jan 17;18(1):21. doi: 10.1186/s13104-024-07051-9. BMC Res Notes. 2025. PMID: 39825399 Free PMC article.
References
-
- Duke BOL. Human onchocerciasis - an overview of the disease. Acta Leiden. 1990;59(1–2):9–24. - PubMed
-
- Bradley JE, Whitworth J, Basáñez MG. In: Topley and Wilson’s Microbiology and Microbial Infections. 10. Wakelin D, Cox F, Despommier D, Gillespie S, editor. London: Edward Arnold Publishers Ltd; 2005. Chapter 39: Onchocerciasis; pp. 781–801.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
