

Circulating cytokines in predicting development of severe acute pancreatitis
- PMID: 24886762
- PMCID: PMC4095695
- DOI: 10.1186/cc13885
Circulating cytokines in predicting development of severe acute pancreatitis
Abstract
Introduction: Severe acute pancreatitis (AP) is associated with high morbidity and mortality. Early prediction of severe AP is needed to improve patient outcomes. The aim of the present study was to find novel cytokines or combinations of cytokines that can be used for the early identification of patients with AP at risk for severe disease.
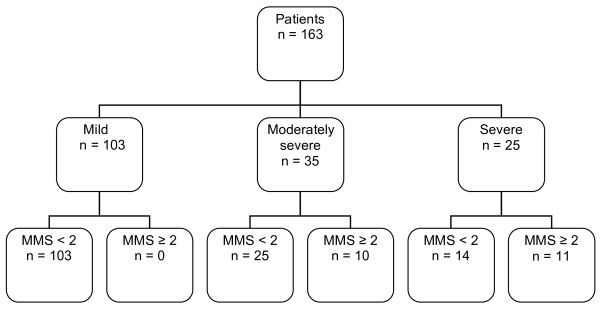
Methods: We performed a prospective study of 163 nonconsecutive patients with AP, of whom 25 had severe AP according to the revised Atlanta criteria. Admission serum levels of 48 cytokines and growth factors were determined using Bio-Plex Pro Human Cytokine Assay 21-plex and 27-plex magnetic bead suspension panels. Admission plasma levels of C-reactive protein (CRP), creatinine and calcium were measured for comparison. In subgroup analyses, we assessed the cytokine profiles of patients with severe AP (n = 14) who did not have organ dysfunction (OD) upon admission (modified Marshall score <2).
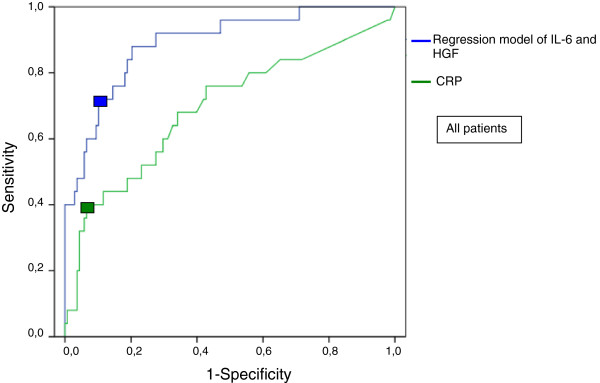
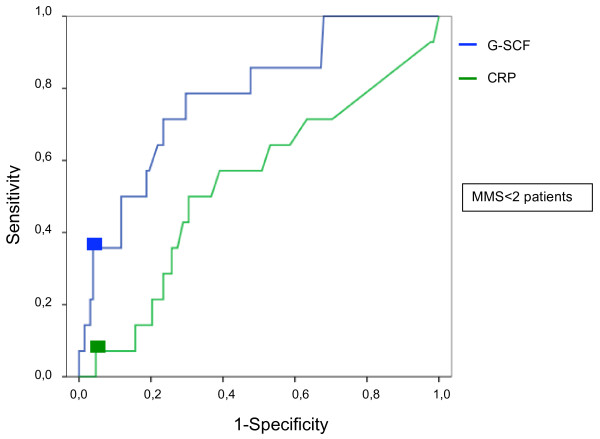
Results: Of 14 cytokines elevated in the severe AP group, interleukin 6 (IL-6) and hepatocyte growth factor (HGF) levels were independent prognostic markers of severe AP. IL-6, HGF and a combination of them predicted severe AP with sensitivities of 56.0%, 60.0% and 72.0%, respectively, and specificities of 90.6%, 92.8% and 89.9%, respectively. The corresponding positive likelihood ratio (LR+) values were 5.9, 8.3 and 7.1, respectively. The predictive values of CRP, creatinine and calcium were comparable to those of the cytokines. In subgroup analyses of patients with severe AP and without OD upon admission, we found that IL-8, HGF and granulocyte colony-stimulating factor (G-CSF) levels predicted the development of severe AP, with G-CSF being the most accurate cytokine at a sensitivity of 35.7%, a specificity of 96.1% and a LR+ of 9.1.
Conclusions: IL-6 and HGF levels upon admission have prognostic value for severe AP which is similar to levels of CRP, creatinine and calcium. Although IL-6 and HGF, as either single or combined markers, were not perfect in identifying patients at risk for severe AP, the possibility that combining them with novel prognostic markers other than cytokines might improve prognostic accuracy needs to be studied. The accuracy of IL-8, HGF and G-CSF levels in predicting severe AP in patients without clinical signs of OD upon admission warrants larger studies.
Figures
Comment in
-
Circulating cytokines in predicting development of severe acute pancreatitis.Crit Care. 2014 Oct 20;18(5):575. doi: 10.1186/s13054-014-0575-0. Crit Care. 2014. PMID: 25673030 Free PMC article.
References
-
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS. Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. doi: 10.1136/gutjnl-2012-302779. - DOI - PubMed
-
- Vege SS, Gardner TB, Chari ST, Munukuti P, Pearson RK, Clain JE, Petersen BT, Baron TH, Farnell MB, Sarr MG. Low mortality and high morbidity in severe acute pancreatitis without organ failure: a case for revising the Atlanta classification to include “moderately severe acute pancreatitis.”. Am J Gastroenterol. 2009;104:710–715. doi: 10.1038/ajg.2008.77. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
