

Age and decisions to limit life support for patients with acute lung injury: a prospective cohort study
- PMID: 24886945
- PMCID: PMC4075260
- DOI: 10.1186/cc13890
Age and decisions to limit life support for patients with acute lung injury: a prospective cohort study
Abstract
Introduction: The proportion of elderly Americans admitted to the intensive care unit (ICU) in the last month of life is rising. Hence, challenging decisions regarding the appropriate use of life support are increasingly common. The objective of this study was to estimate the association between patient age and the rate of new limitations in the use of life support, independent of daily organ dysfunction status, following acute lung injury (ALI) onset.
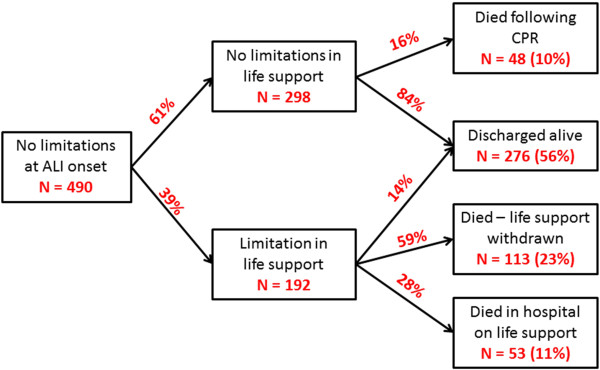
Methods: This was a prospective cohort study of 490 consecutive patients without any limitations in life support at the onset of ALI. Patients were recruited from 11 ICUs at three teaching hospitals in Baltimore, Maryland, USA, and monitored for the incidence of six pre-defined limitations in life support, with adjustment for baseline comorbidity and functional status, duration of hospitalization before ALI onset, ICU severity of illness, and daily ICU organ dysfunction score.
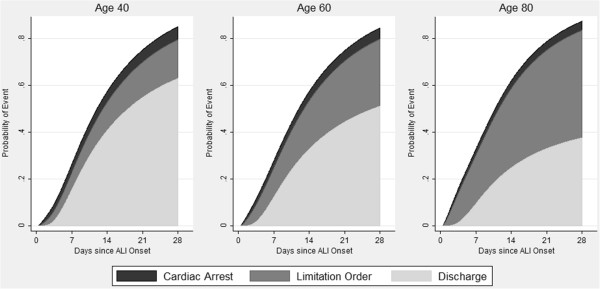
Results: The median patient age was 52 (range: 18 to 96), with 192 (39%) having a new limitation in life support in the ICU. Of patients with a new limitation, 113 (59%) had life support withdrawn and died, 53 (28%) died without resuscitation, and 26 (14%) survived to ICU discharge. Each ten-year increase in patient age was independently associated with a 24% increase in the rate of limitations in life support (Relative Hazard 1.24; 95% CI 1.11 to 1.40) after adjusting for daily ICU organ dysfunction score and all other covariates.
Conclusions: Older critically ill patients are more likely to have new limitations in life support independent of their baseline status, ICU-related severity of illness, and daily organ dysfunction status. Future studies are required to determine whether this association is a result of differences in patient preferences by age, or differences in the treatment options discussed with the families of older versus younger patients.
Figures
Comment in
-
Considering age when making treatment decisions in the ICU: too little, too much, or just right?Crit Care. 2014 Sep 9;18(5):483. doi: 10.1186/s13054-014-0483-3. Crit Care. 2014. PMID: 25673432 Free PMC article.
References
-
- Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key Indicators of Well-Being. Federal Interagency Forum on Aging-Related Statistics. Washington, DC: US Government Printing Office; 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
