

The effect of prone positioning on mortality in patients with acute respiratory distress syndrome: a meta-analysis of randomized controlled trials
- PMID: 24887034
- PMCID: PMC4075407
- DOI: 10.1186/cc13896
The effect of prone positioning on mortality in patients with acute respiratory distress syndrome: a meta-analysis of randomized controlled trials
Abstract
Introduction: Prone positioning (PP) has been reported to improve the survival of patients with severe acute respiratory distress syndrome (ARDS). However, it is uncertain whether the beneficial effects of PP are associated with positive end-expiratory pressure (PEEP) levels and long durations of PP. In this meta-analysis, we aimed to evaluate whether the effects of PP on mortality could be affected by PEEP level and PP duration and to identify which patients might benefit the most from PP.
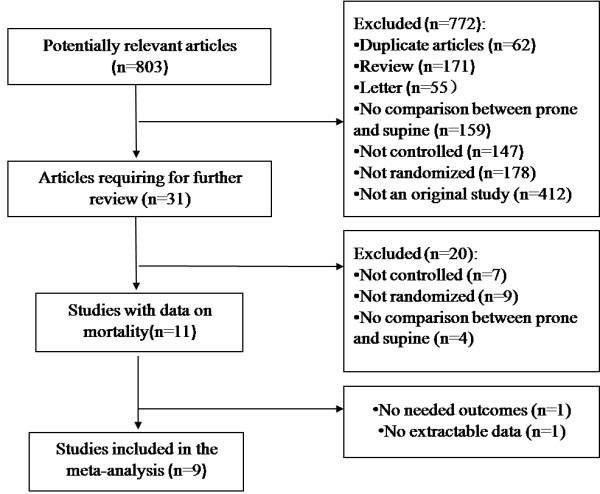
Methods: Publications describing randomized controlled trials (RCTs) in which investigators have compared prone and supine ventilation were retrieved by searching the following electronic databases: PubMed/MEDLINE, the Cochrane Library, the Web of Science and Elsevier Science (inception to May 2013). Two investigators independently selected RCTs and assessed their quality. The data extracted from the RCTs were combined in a cumulative meta-analysis and analyzed using methods recommended by the Cochrane Collaboration.
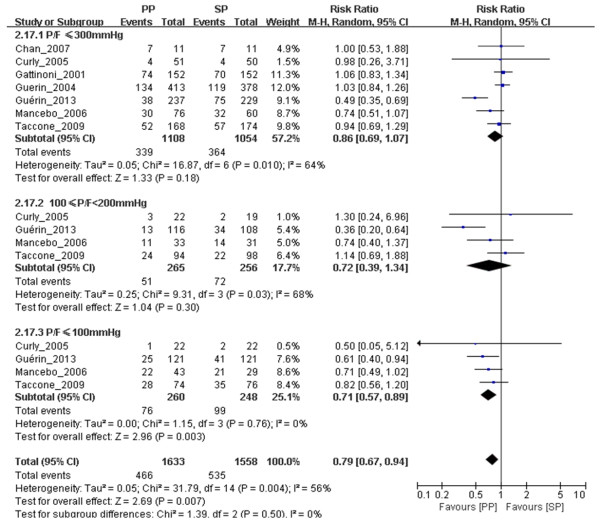
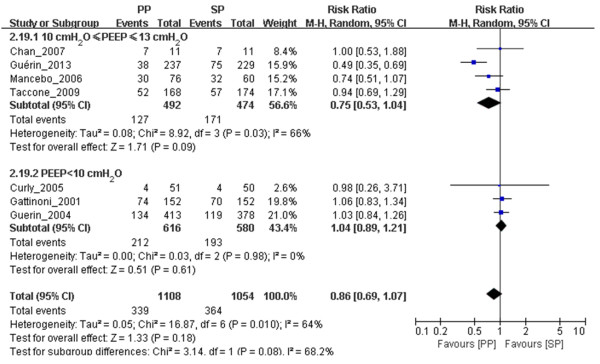
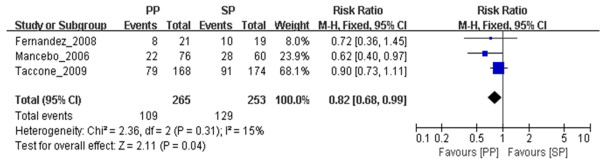
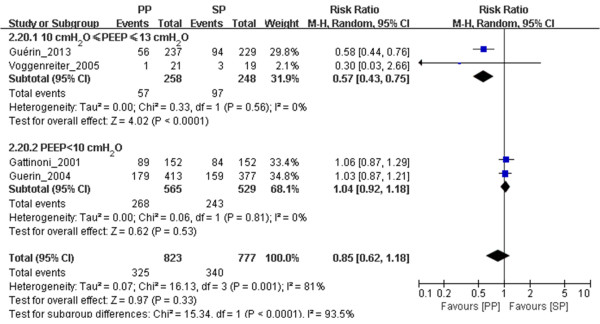
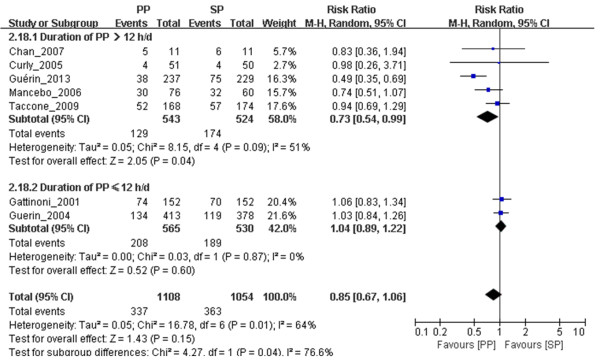
Results: A total of nine RCTs with an aggregate of 2,242 patients were included. All of the studies received scores of up to three points using the methods recommended by Jadad et al. One trial did not conceal allocation. This meta-analysis revealed that, compared with supine positioning, PP decreased the 28- to 30-day mortality of ARDS patients with a ratio of partial pressure of arterial oxygen/fraction of inspired oxygen ≤ 100 mmHg (n = 508, risk ratio (RR) = 0.71, 95 confidence interval (CI) = 0.57 to 0.89; P = 0.003). PP was shown to reduce both 60-day mortality (n = 518, RR = 0.82, 95% CI = 0.68 to 0.99; P = 0.04) and 90-day mortality (n = 516, RR = 0.57, 95% CI = 0.43 to 0.75; P < 0.0001) in ARDS patients ventilated with PEEP ≥ 10 cmH2O. Moreover, PP reduced 28- to 30-day mortality when the PP duration was >12 h/day (n = 1,067, RR = 0.73, 95% CI = 0.54 to 0.99; P = 0.04).
Conclusions: PP reduced mortality among patients with severe ARDS and patients receiving relatively high PEEP levels. Moreover, long-term PP improved the survival of ARDS patients.
Figures
References
-
- Keszler M, Ryckman FC, McDonald JV Jr, Sweet LD, Moront MG, Boegli MJ, Cox C, Leftridge CA. A prospective, multicenter, randomized study of high versus low positive end-expiratory pressure during extracorporeal membrane oxygenation. J Pediatr. 1992;120:107–113. doi: 10.1016/S0022-3476(05)80612-2. - DOI - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Santa Cruz R, Rojas JI, Nervi R, Heredia R, Ciapponi A. High versus low positive end-expiratory pressure (PEEP) levels for mechanically ventilated adult patients with acute lung injury and acute respiratory distress syndrome. Cochrane Database Syst Rev. 2013;6 CD009098. doi:10.1002/14651858. - PMC - PubMed
-
- Tang R, Huang Y, Chen Q, Hui X, Li Y, Yu Q, Zhao H, Yang Y, Qiu H. The effect of alveolar dead space on the measurement of end-expiratory lung volume by modified nitrogen wash-out/wash-in in lavage-induced lung injury. Respir Care. 2012;57:2074–2081. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
