

Effectiveness of a simplified cardiopulmonary resuscitation training program for the non-medical staff of a university hospital
- PMID: 24887037
- PMCID: PMC4024185
- DOI: 10.1186/1757-7241-22-31
Effectiveness of a simplified cardiopulmonary resuscitation training program for the non-medical staff of a university hospital
Abstract
Background: The 2010 Consensus on Science and Treatment Recommendations Statement recommended that short video/computer self-instruction courses, with minimal or no instructor coaching, combined with hands-on practice can be considered an effective alternative to instructor-led basic life support courses. The purpose of this study was to examine the effectiveness of a simplified cardiopulmonary resuscitation (CPR) training program for non-medical staff working at a university hospital.
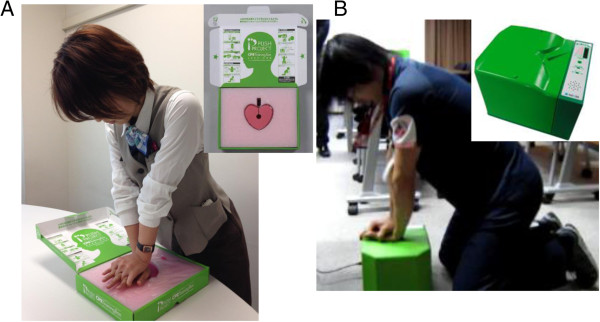
Methods: Before and immediately after a 45-min CPR training program consisting of instruction on chest compression and automated external defibrillator (AED) use with a personal training manikin, CPR skills were automatically recorded and evaluated. Participants' attitudes towards CPR were evaluated by a questionnaire survey.
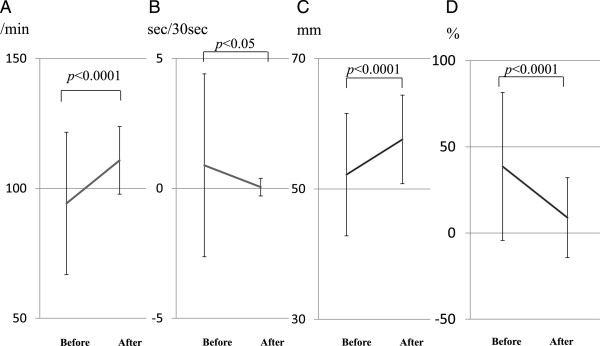
Results: From September 2011 through March 2013, 161 participants attended the program. We evaluated chest compression technique in 109 of these participants. The number of chest compressions delivered after the program versus that before was significantly greater (110.8 ± 13.0/min vs 94.2 ± 27.4/min, p < 0.0001), interruption of chest compressions was significantly shorter (0.05 ± 0.34 sec/30 sec vs 0.89 ± 3.52 sec/30 sec, p < 0.05), mean depth of chest compressions was significantly greater (57.6 ± 6.8 mm vs 52.2 ± 9.4 mm, p < 0.0001), and the proportion of incomplete chest compressions of <5 cm among all chest compressions was significantly decreased (8.9 ± 23.2% vs 38.6 ± 42.9%, p < 0.0001). Of the 159 participants who responded to the questionnaire survey after the program, the proportion of participants who answered 'I can check for a response,' 'I can perform chest compressions,' and 'I can absolutely or I think I can use an AED' increased versus that before the program (81.8% vs 19.5%, 77.4% vs 10.1%, 84.3% vs 23.3%, respectively).
Conclusions: A 45-min simplified CPR training program on chest compression and AED use improved CPR quality and the attitude towards CPR and AED use of non-medical staff of a university hospital.
Figures

Similar articles
-
Long-term retention of cardiopulmonary resuscitation skills after shortened chest compression-only training and conventional training: a randomized controlled trial.Acad Emerg Med. 2014 Jan;21(1):47-54. doi: 10.1111/acem.12293. Acad Emerg Med. 2014. PMID: 24552524 Clinical Trial.
-
"Booster" training: evaluation of instructor-led bedside cardiopulmonary resuscitation skill training and automated corrective feedback to improve cardiopulmonary resuscitation compliance of Pediatric Basic Life Support providers during simulated cardiac arrest.Pediatr Crit Care Med. 2011 May;12(3):e116-21. doi: 10.1097/PCC.0b013e3181e91271. Pediatr Crit Care Med. 2011. PMID: 20625336 Free PMC article. Clinical Trial.
-
Hospital employees improve basic life support skills and confidence with a personal resuscitation manikin and a 24-min video instruction.Resuscitation. 2009 Aug;80(8):898-902. doi: 10.1016/j.resuscitation.2009.06.009. Epub 2009 Jul 1. Resuscitation. 2009. PMID: 19573973
-
2017 American Heart Association Focused Update on Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Circulation. 2018 Jan 2;137(1):e1-e6. doi: 10.1161/CIR.0000000000000540. Epub 2017 Nov 6. Circulation. 2018. PMID: 29114009 Review.
-
Cardiopulmonary resuscitation without ventilation.Crit Care Med. 2000 Nov;28(11 Suppl):N186-9. doi: 10.1097/00003246-200011001-00003. Crit Care Med. 2000. PMID: 11098942 Review.
Cited by
-
The Effect of the Duration of Basic Life Support Training on the Learners' Cardiopulmonary and Automated External Defibrillator Skills.Biomed Res Int. 2016;2016:2420568. doi: 10.1155/2016/2420568. Epub 2016 Jul 27. Biomed Res Int. 2016. PMID: 27529066 Free PMC article. Clinical Trial.
-
A follow-up report on the effect of a simplified basic life support training program for non-medical staff working at a university hospital: changes in attitude toward cardiopulmonary resuscitation and automated external defibrillator use through repeat training.Acute Med Surg. 2020 Aug 6;7(1):e548. doi: 10.1002/ams2.548. eCollection 2020 Jan-Dec. Acute Med Surg. 2020. PMID: 32782811 Free PMC article.
-
Degree of exercise intensity during continuous chest compression in upper-body-trained individuals.J Physiol Anthropol. 2015 Dec 19;34:43. doi: 10.1186/s40101-015-0079-x. J Physiol Anthropol. 2015. PMID: 26687118 Free PMC article.
-
Cardiopulmonary resuscitation (CPR) psychomotor skills of laypeople, as affected by training interventions, number of times trained and retention testing intervals: A dataset derived from a systematic review.Data Brief. 2019 Jul 9;25:104236. doi: 10.1016/j.dib.2019.104236. eCollection 2019 Aug. Data Brief. 2019. PMID: 31497626 Free PMC article.
-
Assessment of long-term impact of formal certified cardiopulmonary resuscitation training program among nurses.Indian J Crit Care Med. 2016 Apr;20(4):226-32. doi: 10.4103/0972-5229.180043. Indian J Crit Care Med. 2016. PMID: 27303137 Free PMC article.
References
-
- Hallstrom AP, Ornato JP, Weisfeldt M, Travers A, Christenson J, McBurnie MA, Zalenski R, Becker LB, Schron EB, Proschan M. Public-access defibrillation and survival after out-of-hospital cardiac arrest. New Engl J Med. 2004;351:637–646. - PubMed
-
- Hazinski MF, Nolan JP, Billi JE, Bottiger BW, Bossaert L, De Caen AR, Deakin CD, Drajer S, Eigel B, Hickey RW, Jacobs I, Kleinman ME, Kloeck W, Koster RW, Lim SH, Mancini ME, Montgomery WH, Morley PT, Morrison LJ, Nadkarni VM, O'Connor RE, Okada K, Perlman JM, Sayre MR, Shuster M, Soar J, Sunde K, Travers AH, Wyllie J, Zideman D. Part 1: Executive summary: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122:S250–S275. doi: 10.1161/CIRCULATIONAHA.110.970897. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
