

Serum cystatin C predicts vancomycin trough levels better than serum creatinine in hospitalized patients: a cohort study
- PMID: 24887089
- PMCID: PMC4075252
- DOI: 10.1186/cc13899
Serum cystatin C predicts vancomycin trough levels better than serum creatinine in hospitalized patients: a cohort study
Abstract
Introduction: Serum cystatin C can improve glomerular filtration rate (GFR) estimation over creatinine alone, but whether this translates into clinically relevant improvements in drug dosing is unclear.
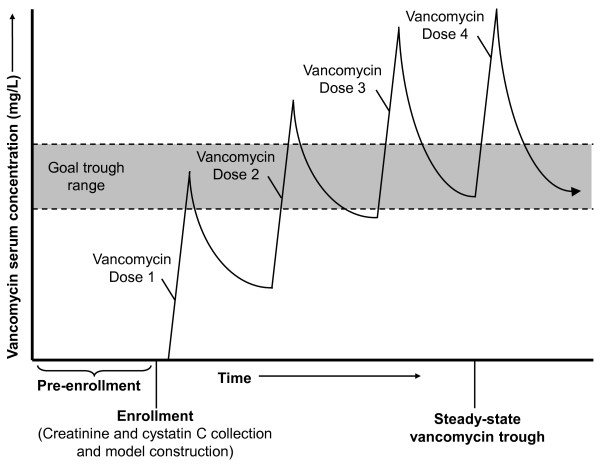
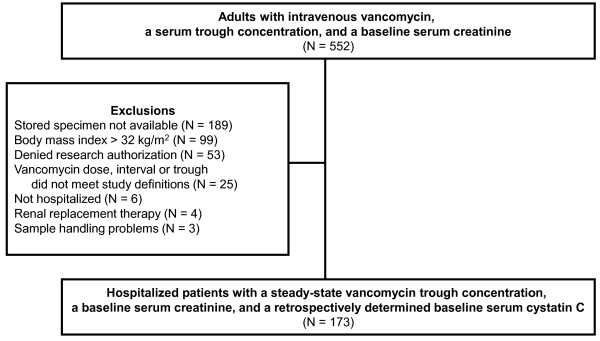
Methods: This prospective cohort study enrolled adults receiving scheduled intravenous vancomycin while hospitalized at the Mayo Clinic in 2012. Vancomycin dosing was based on weight, serum creatinine with the Cockcroft-Gault equation, and clinical judgment. Cystatin C was later assayed from the stored serum used for the creatinine-based dosing. Vancomycin trough prediction models were developed by using factors available at therapy initiation. Residuals from each model were used to predict the proportion of patients who would have achieved the target trough with the model compared with that observed with usual care.
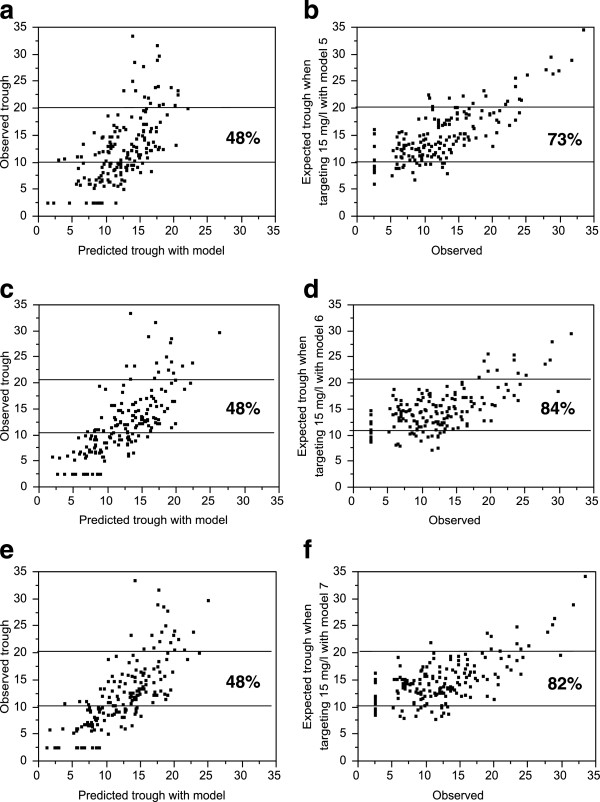
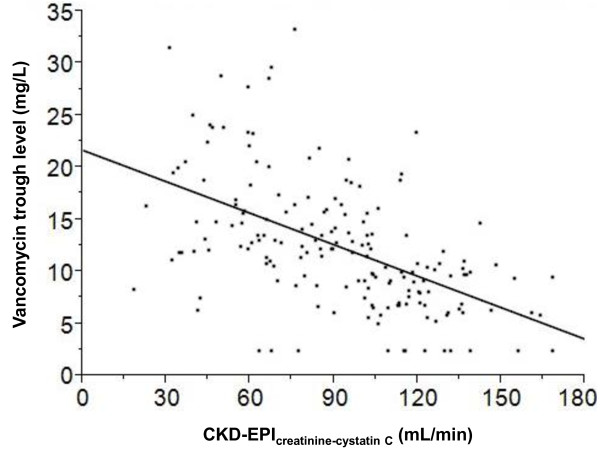
Results: Of 173 patients enrolled, only 35 (20%) had a trough vancomycin level within their target range (10 to 15 mg/L or 15 to 20 mg/L). Cystatin C-inclusive models better predicted vancomycin troughs than models based upon serum creatinine alone, although both were an improvement over usual care. The optimal model used estimated GFR by the Chronic Kidney Disease Epidemiology Collaborative (CKD-EPI) creatinine-cystatin C equation (R(2) = 0.580). This model is expected to yield 54% (95% confidence interval 45% to 61%) target trough attainment (P <0.001 compared with the 20% with usual care).
Conclusions: Vancomycin dosing based on standard care with Cockcroft-Gault creatinine clearance yielded poor trough achievement. The developed dosing model with estimated GFR from CKD-EPIcreatinine-cystatin C could yield a 2.5-fold increase in target trough achievement compared with current clinical practice. Although this study is promising, prospective validation of this or similar cystatin C-inclusive dosing models is warranted.
Figures
Comment in
-
Estimated GFR and cystatin C for drug dosing: moving beyond proof of concept to clinical translation?Am J Kidney Dis. 2015 Apr;65(4):534-6. doi: 10.1053/j.ajkd.2014.11.006. Epub 2014 Dec 24. Am J Kidney Dis. 2015. PMID: 25542411 No abstract available.
Similar articles
-
Cystatin C-Guided Vancomycin Dosing in Critically Ill Patients: A Quality Improvement Project.Am J Kidney Dis. 2017 May;69(5):658-666. doi: 10.1053/j.ajkd.2016.11.016. Epub 2017 Jan 25. Am J Kidney Dis. 2017. PMID: 28131530 Clinical Trial.
-
Comparison of the Predictive Performance Between Cystatin C and Serum Creatinine by Vancomycin via a Population Pharmacokinetic Models: A Prospective Study in a Chinese Population.Eur J Drug Metab Pharmacokinet. 2020 Feb;45(1):135-149. doi: 10.1007/s13318-019-00578-4. Eur J Drug Metab Pharmacokinet. 2020. PMID: 31541402
-
Serum cystatin C for the prediction of glomerular filtration rate with regard to the dose adjustment of amikacin, gentamicin, tobramycin, and vancomycin.Ther Drug Monit. 2006 Jun;28(3):326-31. doi: 10.1097/01.ftd.0000211805.89440.3d. Ther Drug Monit. 2006. PMID: 16778715
-
Prediction of the Renal Elimination of Drugs With Cystatin C vs Creatinine: A Systematic Review.Mayo Clin Proc. 2019 Mar;94(3):500-514. doi: 10.1016/j.mayocp.2018.08.002. Epub 2019 Jan 31. Mayo Clin Proc. 2019. PMID: 30713050
-
Calibration and precision of serum creatinine and plasma cystatin C measurement: impact on the estimation of glomerular filtration rate.J Nephrol. 2014 Oct;27(5):467-75. doi: 10.1007/s40620-014-0087-7. Epub 2014 Apr 8. J Nephrol. 2014. PMID: 24711159 Review.
Cited by
-
Sarcopenia Index Is a Simple Objective Screening Tool for Malnutrition in the Critically Ill.JPEN J Parenter Enteral Nutr. 2019 Aug;43(6):780-788. doi: 10.1002/jpen.1492. Epub 2018 Dec 18. JPEN J Parenter Enteral Nutr. 2019. PMID: 30561031 Free PMC article.
-
Cystatin C may be better than creatinine for digoxin dosing in older adults with atrial fibrillation.J Clin Lab Anal. 2020 Oct;34(10):e23427. doi: 10.1002/jcla.23427. Epub 2020 Jun 17. J Clin Lab Anal. 2020. PMID: 32716587 Free PMC article.
-
Prediction of Vancomycin Levels Using Cystatin C in Overweight and Obese Patients: a Retrospective Cohort Study of Hospitalized Patients.Antimicrob Agents Chemother. 2020 Dec 16;65(1):e01487-20. doi: 10.1128/AAC.01487-20. Print 2020 Dec 16. Antimicrob Agents Chemother. 2020. PMID: 33106257 Free PMC article.
-
Medication Management in the Critically Ill Patient with Acute Kidney Injury.Clin J Am Soc Nephrol. 2023 Aug;18(8):1080-1088. doi: 10.2215/CJN.0000000000000101. Epub 2023 Feb 1. Clin J Am Soc Nephrol. 2023. PMID: 36723347 Free PMC article. Review.
-
Precision medication based on the evaluation of drug metabolizing enzyme and transporter functions.Precis Clin Med. 2025 Feb 22;8(1):pbaf004. doi: 10.1093/pcmedi/pbaf004. eCollection 2025 Mar. Precis Clin Med. 2025. PMID: 40110576 Free PMC article. Review.
References
-
- Levine DP. Vancomycin: a history. Clin Infect Dis. 2006;42:S5–S12. - PubMed
-
- Ena J, Dick RW, Jones RN, Wenzel RP. The epidemiology of intravenous vancomycin usage in a university hospital. A 10-year study. JAMA. 1993;269:598–602. - PubMed
-
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, Rybak MJ, Talan DA, Chambers HF. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52:285–292. - PubMed
-
- Rybak M, Lomaestro B, Rotschafer JC, Moellering R Jr, Craig W, Billeter M, Dalovisio JR, Levine DP. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm. 2009;66:82–98. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
