

Cost and Mortality Associated With Postoperative Acute Kidney Injury
- PMID: 24887982
- PMCID: PMC4247993
- DOI: 10.1097/SLA.0000000000000732
Cost and Mortality Associated With Postoperative Acute Kidney Injury
Abstract
Objective: To determine the incremental hospital cost and mortality associated with the development of postoperative acute kidney injury (AKI) and with other associated postoperative complications.
Background: Each year 1.5 million patients develop a major complication after surgery. Postoperative AKI is one of the most common postoperative complications and is associated with an increase in hospital mortality and decreased survival for up to 15 years after surgery.
Methods: In a single-center cohort of 50,314 adult surgical patients undergoing major inpatient surgery, we applied risk-adjusted regression models for cost and mortality using postoperative AKI and other complications as the main independent predictors. We defined AKI using consensus Risk, Injury, Failure, Loss and End-Stage Renal Disease criteria.
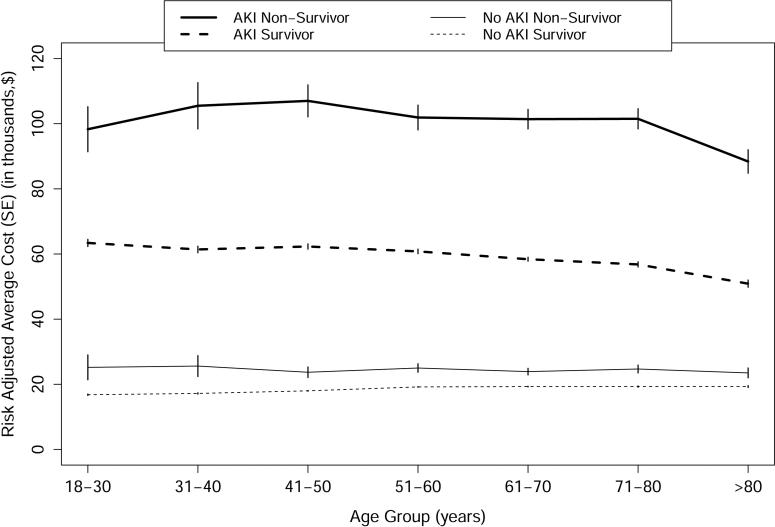
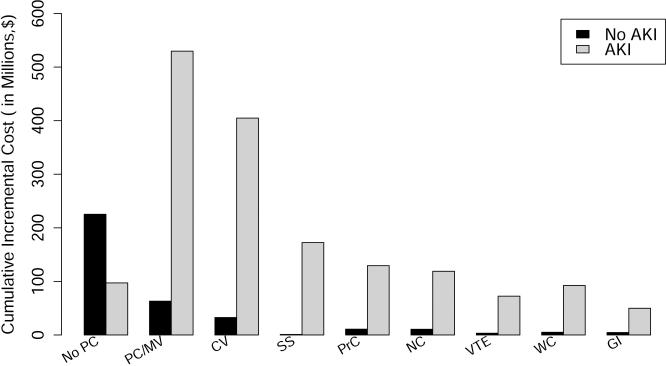
Results: The prevalence of AKI was 39% among 50,314 patients with available serum creatinine. Patients with AKI were more likely to have postoperative complications and had longer lengths of stay in the intensive care unit and the hospital. The risk-adjusted average cost of care for patients undergoing surgery was $42,600 for patients with any AKI compared with $26,700 for patients without AKI. The risk-adjusted 90-day mortality was 6.5% for patients with any AKI compared with 4.4% for patients without AKI. Serious postoperative complications resulted in increased cost of care and mortality for all patients, but the increase was much larger for those patients with any degree of AKI.
Conclusions: Hospital costs and mortality are strongly associated with postoperative AKI, are correlated with the severity of AKI, and are much higher for patients with other postoperative complications in addition to AKI.
Figures
References
-
- Lee PH, Gawande AA. The number of surgical procedures in an American lifetime in 3 states. J Am Coll Surg. 2008;207:S75–S75.
-
- Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. The Lancet. 372:139–144. - PubMed
-
- Dimick JB, Weeks WB, Karia RJ, et al. Who pays for poor surgical quality? Building a business case for quality improvement. J Am Coll Surg. 2006;202:933–7. - PubMed
-
- Hall BL, Hamilton BH, Richards K, et al. Does Surgical Quality Improve in the American College of Surgeons National Surgical Quality Improvement Program: An Evaluation of All Participating Hospitals. Ann Surg. 2009;250:363–376. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
