

Compliance with referrals for non-acute child health conditions: evidence from the longitudinal ASENZE study in KwaZulu Natal, South Africa
- PMID: 24888212
- PMCID: PMC4067123
- DOI: 10.1186/1472-6963-14-242
Compliance with referrals for non-acute child health conditions: evidence from the longitudinal ASENZE study in KwaZulu Natal, South Africa
Abstract
Background: Caregiver compliance with referrals for child health services is essential to child health outcomes. Many studies in sub-Saharan Africa have examined compliance patterns for children referred for acute, life-threatening conditions but few for children referred for non-acute conditions. The aims of this analysis were to determine the rate of referral compliance and investigate factors associated with referral compliance in KwaZulu Natal, South Africa.
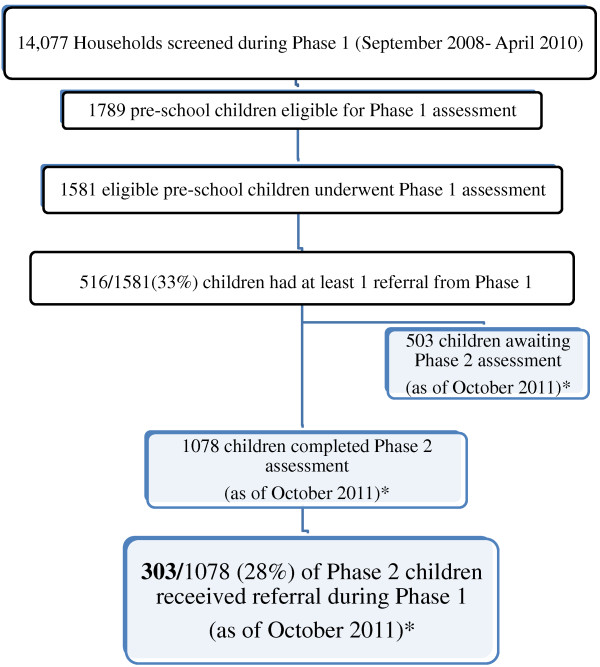
Methods: From September 2008-2010, a door-to-door household survey was conducted to identify children aged 4-6 years in outer-west eThekwini District, KwaZulu-Natal, South Africa. Of 2,049 identified, informed consent was obtained for 1787 (89%) children who were then invited for baseline assessments. 1581 children received standardized medical and developmental assessments at the study facility (Phase 1). Children with anemia, suspected disorders of vision, hearing, behavior and/or development and positive HIV testing were referred to local health facilities. Caregiver-reported compliance with referrals was assessed 18-24 months later (Phase 2). Relationships between socio-demographic factors and referral compliance were evaluated using chi-square tests.
Results: Of 1581 children, 516 received referrals for ≥1 non-acute conditions. At the time of analysis, 68% (1078 /1581) returned for Phase 2. Analysis was limited to children assessed in Phase 2 who received a referral in Phase 1 (n = 303). Common referral reasons were suspected disorders of hearing/middle ear (22%), visual acuity (12%) and anemia (14%). Additionally, children testing positive for HIV (6.6%) were also referred. Of 303 children referred, only 45% completed referrals. Referral compliance was low for suspected disorders of vision, hearing and development. Referral compliance was significantly lower for children with younger caregivers, those living in households with low educational attainment and for those with unstable caregiving.
Conclusions: Compliance with referrals for children with non-acute conditions is low within this population and appears to be influenced by caregiver age, household education level and stability of caregiving. Lack of treatment for hearing, vision and developmental problems can contribute to long-term cognitive difficulties. Further research is underway by this group to examine caregiver knowledge and attitudes about referral conditions and health system characteristics as potential determinants of referral compliance.
Figures
References
-
- Maulik PK, Darmstadt GL. Childhood disability in low- and middle-income countries: overview of screening, prevention, services, legislation, and epidemiology. Pediatrics. 2007;14(Suppl 1):S1–S55. - PubMed
-
- Bossyns P, Abache R, Abdoulaye MS, Miye H, Depoorter AM, Van Lerberghe W. Monitoring the referral system through benchmarking in rural Niger: an evaluation of the functional relation between health centres and the district hospital. BMC Health Serv Res. 2006;14:51. doi: 10.1186/1472-6963-6-51. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
