

Venous thromboembolic prophylaxis after a hepatic resection: patterns of care among liver surgeons
- PMID: 24888461
- PMCID: PMC4238855
- DOI: 10.1111/hpb.12278
Venous thromboembolic prophylaxis after a hepatic resection: patterns of care among liver surgeons
Abstract
Introduction: No consensus exists for post-hepatectomy venous thromboembolic (VTE) prophylaxis. Factors impacting VTE prophylaxis patterns among hepato-pancreato-biliary (HPB) surgeons were defined.
Method: Surgeons were invited to complete a web-based survey on VTE prophylaxis. The impact of physician and clinical factors was analysed.
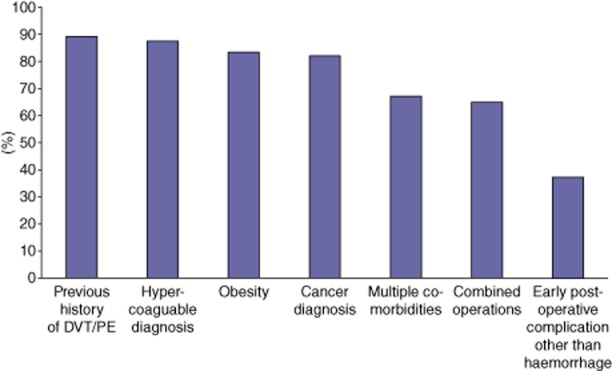
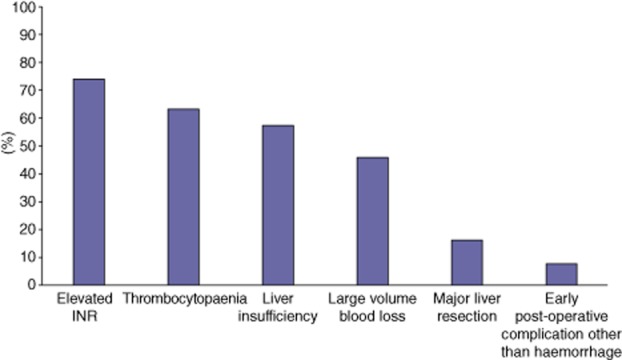
Results: Two hundred responses were received. Most respondents were male (91%) and practiced at academic centres (88%) in the United States (80%). Surgical training varied: HPB (24%), transplantation (24%), surgical oncology (34%), HPB/transplantation (13%), or no specialty (5%). Respondents estimated VTE risk was higher after major (6%) versus minor (3%) resections. Although 98% use VTE prophylaxis, there was considerable variability: sequential compression devices (SCD) (91%), unfractionated heparin Q12h (31%) and Q8h (32%), and low-molecular weight heparin (39%). While 88% noted VTE prophylaxis was not impacted by operative indication, 16% stated major resections reduced their VTE prophylaxis. Factors associated with the decreased use of pharmacologic prophylaxis included: elevated international normalized ratio (INR) (74%), thrombocytopaenia (63%), liver insufficiency (58%), large EBL (46%) and complications (8%). Forty-seven per cent of respondents wait until ≥post-operative day 1 (POD1) and 35% hold pharmacologic VTE prophylaxis until no signs of coagulopathy. A minority (14%) discharge patients on pharmacologic prophylaxis. While 81% have institutional VTE guidelines, 79% believe hepatectomy-specific guidelines would be helpful.
Conclusion: There is considerable variation regarding VTE prophylaxis among liver surgeons. While most HPB surgeons employ VTE prophylaxis, the methods, timing and purported contraindications differ significantly.
© 2014 International Hepato-Pancreato-Biliary Association.
Figures
Similar articles
-
Perception of Chemical Venous Thromboprophylaxis for Oncologic Lung Resections among Thoracic Surgeons.Ann Vasc Surg. 2017 Oct;44:299-306. doi: 10.1016/j.avsg.2017.03.188. Epub 2017 May 5. Ann Vasc Surg. 2017. PMID: 28479450
-
Practice patterns of VTE chemoprophylaxis after discharge following hepatic and pancreatic resections for cancer: A survey of hepatopancreatobiliary surgeons.J Thromb Thrombolysis. 2019 Jul;48(1):119-124. doi: 10.1007/s11239-019-01834-9. J Thromb Thrombolysis. 2019. PMID: 30877618 Free PMC article.
-
Identification of patients at high risk for post-discharge venous thromboembolism after hepato-pancreato-biliary surgery: which patients benefit from extended thromboprophylaxis?HPB (Oxford). 2018 Jul;20(7):621-630. doi: 10.1016/j.hpb.2018.01.004. Epub 2018 Feb 19. HPB (Oxford). 2018. PMID: 29472105
-
Asian venous thromboembolism guidelines: prevention of venous thromboembolism.Int Angiol. 2012 Dec;31(6):501-16. Int Angiol. 2012. PMID: 23222928 Review.
-
Venous Thromboembolism Quality Measures Fail to Accurately Measure Quality.Circulation. 2018 Mar 20;137(12):1278-1284. doi: 10.1161/CIRCULATIONAHA.116.026897. Circulation. 2018. PMID: 29555709 Review.
Cited by
-
Dabigatran (Pradaxa) Is Safe for Extended Venous Thromboembolism Prophylaxis After Surgery for Pancreatic Cancer.J Gastrointest Surg. 2019 Jun;23(6):1166-1171. doi: 10.1007/s11605-018-3936-1. Epub 2018 Sep 5. J Gastrointest Surg. 2019. PMID: 30187331
-
Venous thromboembolism and bleeding after hepatectomy: role and impact of risk adjusted prophylaxis.J Thromb Thrombolysis. 2023 Oct;56(3):375-387. doi: 10.1007/s11239-023-02847-1. Epub 2023 Jun 23. J Thromb Thrombolysis. 2023. PMID: 37351821
-
Evaluation of perioperative routine coagulation testing versus thromboelastography for major liver resection - A single-arm, prospective, interventional trial (PORTAL trial).Indian J Anaesth. 2023 Dec;67(12):1077-1083. doi: 10.4103/ija.ija_344_23. Epub 2023 Dec 13. Indian J Anaesth. 2023. PMID: 38343681 Free PMC article.
-
Association Between Operative Approach and Venous Thromboembolism Rate Following Hepatectomy: a Propensity-Matched Analysis.J Gastrointest Surg. 2021 Nov;25(11):2778-2787. doi: 10.1007/s11605-020-04887-x. Epub 2020 Nov 24. J Gastrointest Surg. 2021. PMID: 33236321
-
Development and validation of a risk calculator for post-discharge venous thromboembolism following hepatectomy for malignancy.HPB (Oxford). 2021 May;23(5):723-732. doi: 10.1016/j.hpb.2020.09.008. Epub 2020 Sep 26. HPB (Oxford). 2021. PMID: 32988755 Free PMC article.
References
-
- Collins R, Scrimgeour A, Yusuf S, Peto R. Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration of subcutaneous heparin. Overview of results of randomized trials in general, orthopedic, and urologic surgery. N Engl J Med. 1988;318:1162–1173. - PubMed
-
- Mismetti P, Laporte S, Darmon JY, Buchmuller A, Decousus H. Meta-analysis of low molecular weight heparin in the prevention of venous thromboembolism in general surgery. Br J Surg. 2001;88:913–930. - PubMed
-
- Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al. Prevention of VTE in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S–e277S. - PMC - PubMed
-
- Lyman GH, Khorana AA, Kuderer NM, Lee AY, Arcelus JI, Balaban EP, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013;31:2189–2204. - PubMed
-
- Caprini JA, Arcelus JI, Hasty JH, Tamhane AC, Fabrega F. Clinical assessment of venous thromboembolic risk in surgical patients. Semin Thromb Hemost. 1991;17(Suppl 3):304–312. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
