

Interrater agreement for Critical Care EEG Terminology
- PMID: 24888711
- PMCID: PMC4879939
- DOI: 10.1111/epi.12653
Interrater agreement for Critical Care EEG Terminology
Abstract
Objective: The interpretation of critical care electroencephalography (EEG) studies is challenging because of the presence of many periodic and rhythmic patterns of uncertain clinical significance. Defining the clinical significance of these patterns requires standardized terminology with high interrater agreement (IRA). We sought to evaluate IRA for the final, published American Clinical Neurophysiology Society (ACNS)-approved version of the critical care EEG terminology (2012 version). Our evaluation included terms not assessed previously and incorporated raters with a broad range of EEG reading experience.
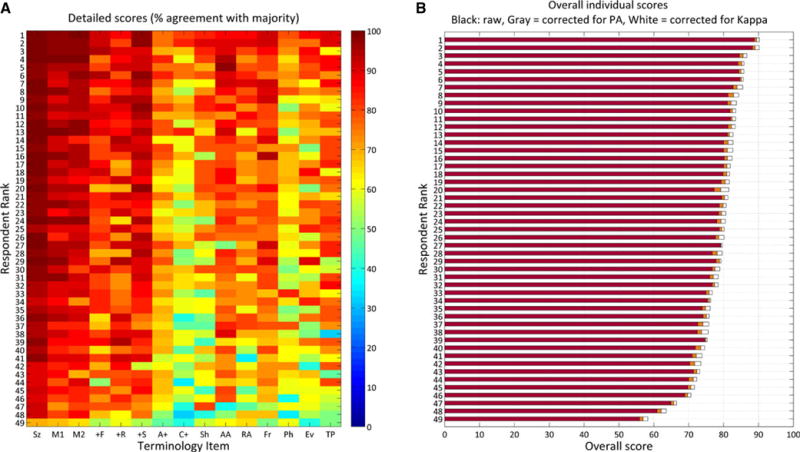
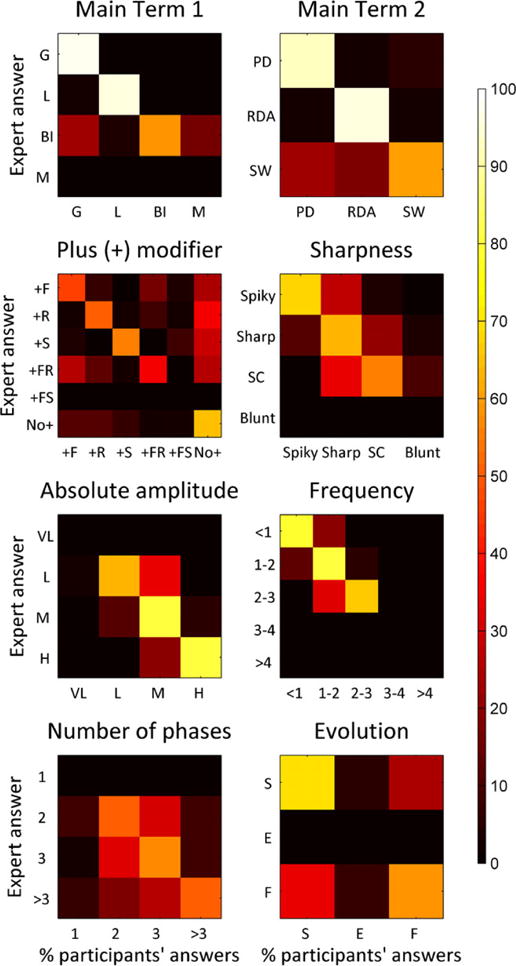
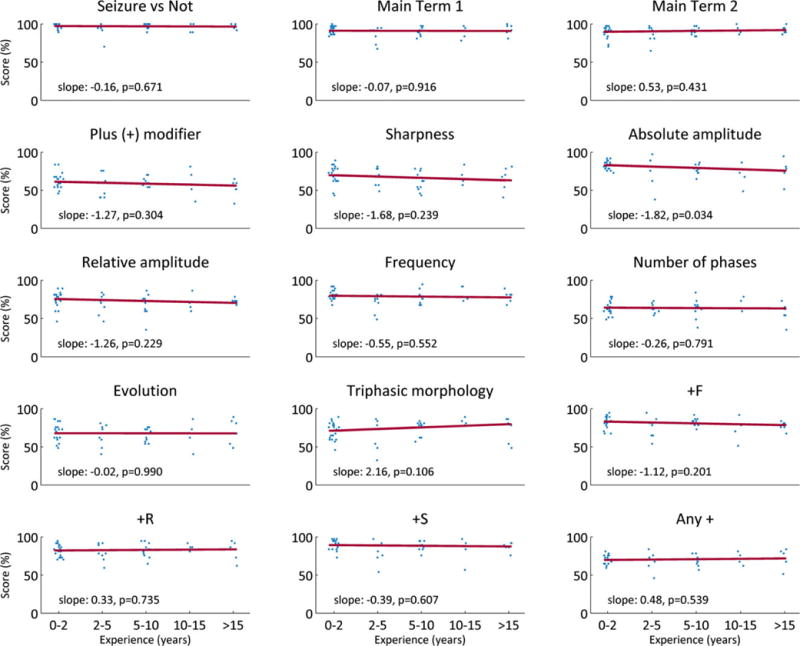
Methods: After reviewing a set of training slides, 49 readers independently completed a Web-based test consisting of 11 identical questions for each of 37 EEG samples (407 questions). Questions assessed whether a pattern was an electrographic seizure; pattern location (main term 1), pattern type (main term 2); and presence and classification of eight other key features ("plus" modifiers, sharpness, absolute and relative amplitude, frequency, number of phases, fluctuation/evolution, and the presence of "triphasic" morphology).
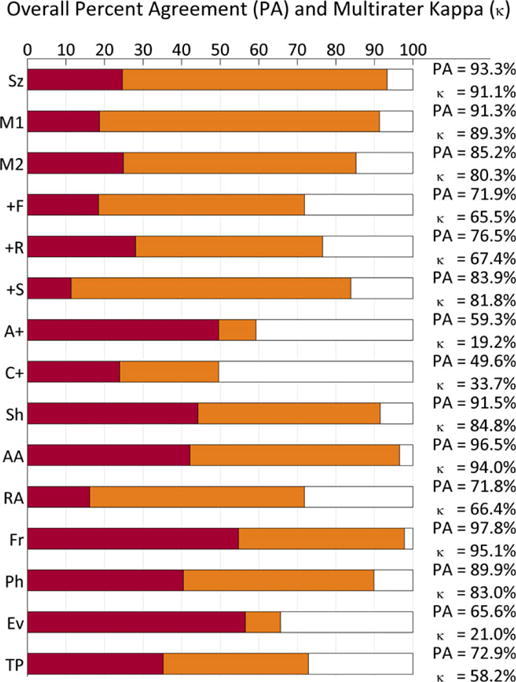
Results: IRA statistics (κ values) were almost perfect (90-100%) for seizures, main terms 1 and 2, the +S modifier (superimposed spikes/sharp waves or sharply contoured rhythmic delta activity), sharpness, absolute amplitude, frequency, and number of phases. Agreement was substantial for the +F (superimposed fast activity) and +R (superimposed rhythmic delta activity) modifiers (66% and 67%, respectively), moderate for triphasic morphology (58%), and fair for evolution (21%).
Significance: IRA for most terms in the ACNS critical care EEG terminology is high. These terms are suitable for multicenter research on the clinical significance of critical care EEG patterns. A PowerPoint slide summarizing this article is available for download in the Supporting Information section http://dx.doi.org/10.1111/epi.12653/supinfo.
Keywords: Continuous EEG monitoring; Critical care; EEG terminology; GPEDs; Intensive care; Interrater agreement; PLEDs; Periodic patterns; Rhythmic patterns.
Wiley Periodicals, Inc. © 2014 International League Against Epilepsy.
Conflict of interest statement
All authors are members of the CCEMRC. The CCEMRC received infrastructure support from the American Epilepsy Society/Epilepsy Foundation. NG received support from the Epilepsy Foundation. LJH received research support for investigator-initiated studies from UCB-Pharma, Upsher-Smith, and Lundbeck; consultation fees for advising from Lund-beck, Upsher-Smith, GlaxoSmithKline RSC Diagnostics, and NeuroPace; royalties for authoring chapters for UpToDate-Neurology, and for coauthoring the book
Figures
References
-
- Chong DJ, Hirsch LJ. Which EEG patterns warrant treatment in the critically ill? Reviewing the evidence for treatment of periodic epileptiform discharges and related patterns. J Clin Neurophysiol. 2005;22:79–91. - PubMed
-
- Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17:3–23. - PubMed
-
- Orta DSJ, Chiappa KH, Quiroz AZ, et al. Prognostic implications of periodic epileptiform discharges. Arch Neurol. 2009;66:985–991. - PubMed
-
- Claassen J, Taccone FS, Horn P, et al. Recommendations on the use of EEG monitoring in critically ill patients: consensus statement from the neurointensive care section of the ESICM. Intensive Care Med. 2013;39:1337–1351. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
