

How successful is Medicare Advantage?
- PMID: 24890251
- PMCID: PMC4089375
- DOI: 10.1111/1468-0009.12061
How successful is Medicare Advantage?
Abstract
Context: Medicare Part C, or Medicare Advantage (MA), now almost 30 years old, has generally been viewed as a policy disappointment. Enrollment has vacillated but has never come close to the penetration of managed care plans in the commercial insurance market or in Medicaid, and because of payment policy decisions and selection, the MA program is viewed as having added to cost rather than saving funds for the Medicare program. Recent changes in Medicare policy, including improved risk adjustment, however, may have changed this picture.
Methods: This article summarizes findings from our group's work evaluating MA's recent performance and investigating payment options for improving its performance even more. We studied the behavior of both beneficiaries and plans, as well as the effects of Medicare policy.
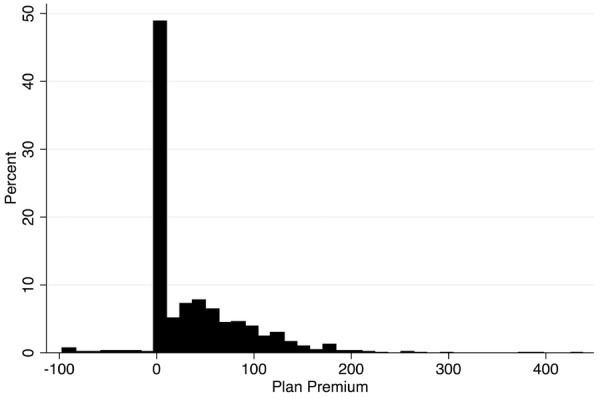
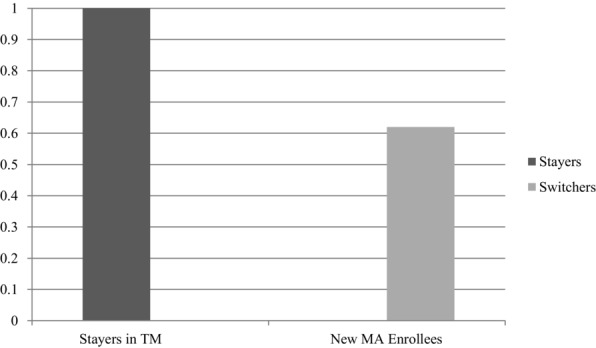
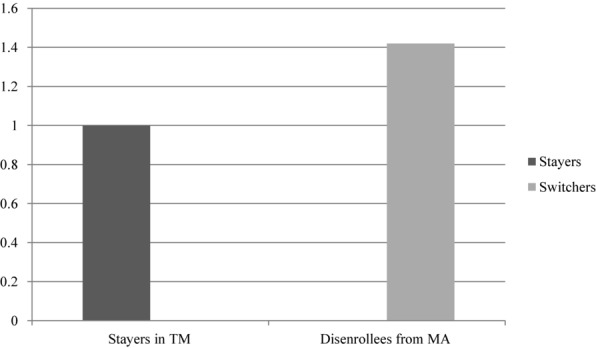
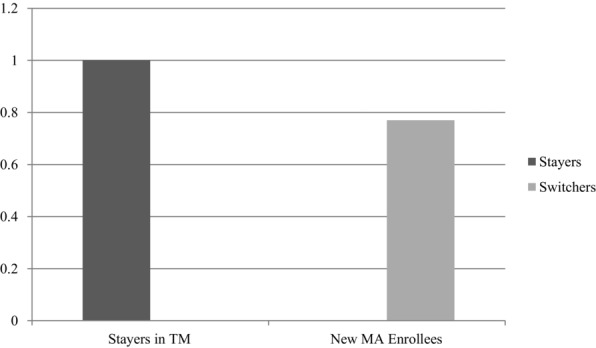
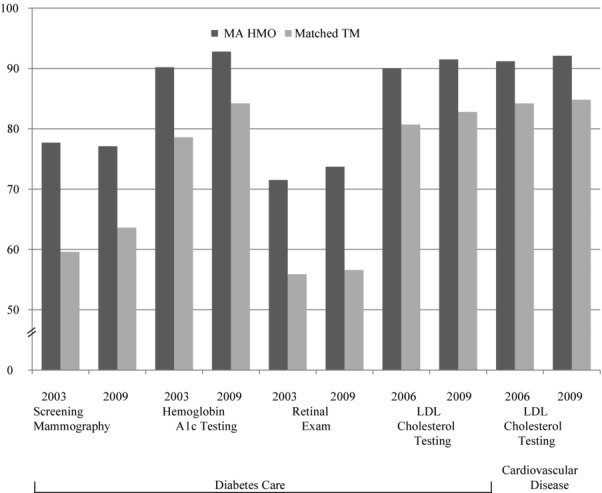
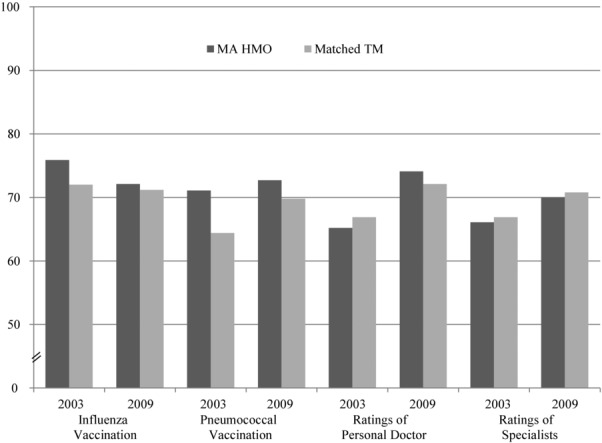
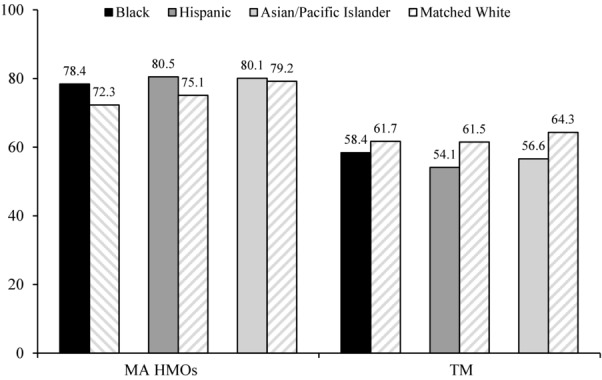
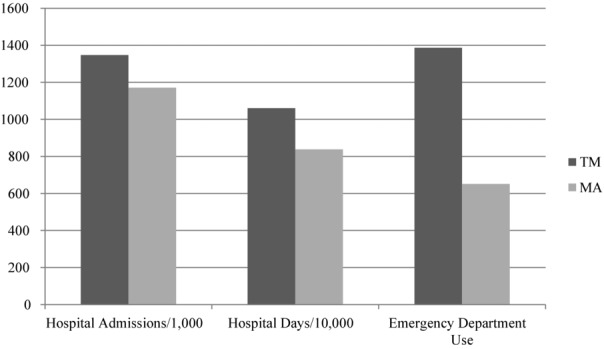
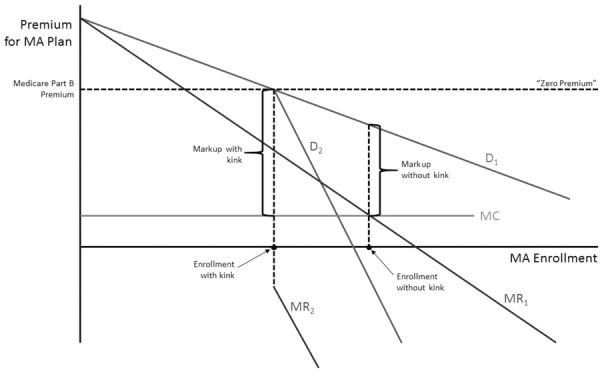
Findings: Beneficiaries make "mistakes" in their choice of MA plan options that can be explained by behavioral economics. Few beneficiaries make an active choice after they enroll in Medicare. The high prevalence of "zero-premium" plans signals inefficiency in plan design and in the market's functioning. That is, Medicare premium policies interfere with economically efficient choices. The adverse selection problem, in which healthier, lower-cost beneficiaries tend to join MA, appears much diminished. The available measures, while limited, suggest that, on average, MA plans offer care of equal or higher quality and for less cost than traditional Medicare (TM). In counties, greater MA penetration appears to improve TM's performance.
Conclusions: Medicare policies regarding lock-in provisions and risk adjustment that were adopted in the mid-2000s have mitigated the adverse selection problem previously plaguing MA. On average, MA plans appear to offer higher value than TM, and positive spillovers from MA into TM imply that reimbursement should not necessarily be neutral. Policy changes in Medicare that reform the way that beneficiaries are charged for MA plan membership are warranted to move more beneficiaries into MA.
Keywords: Medicare; health care costs; managed care; payment policy.
© 2014 Milbank Memorial Fund.
Figures
References
-
- Gold M, Jacobson G, D'Amico A, Neuman T. Medicare Advantage 2013 spotlight: enrollment market update http://kaiserfamilyfoundation.files.wordpress.com/2013/06/8448.pdf. Published June 2013. Accessed September 7, 2013.
-
- Centers for Medicare and Medicaid Services. CMS fast facts http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trend.... Updated January 15, 2014. Accessed February 5, 2014. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
