

Upper abdominal normal organ contouring guidelines and atlas: a Radiation Therapy Oncology Group consensus
- PMID: 24890348
- PMCID: PMC4285338
- DOI: 10.1016/j.prro.2013.06.004
Upper abdominal normal organ contouring guidelines and atlas: a Radiation Therapy Oncology Group consensus
Abstract
Purpose: To standardize upper abdominal normal organ contouring guidelines for Radiation Therapy Oncology Group (RTOG) trials.
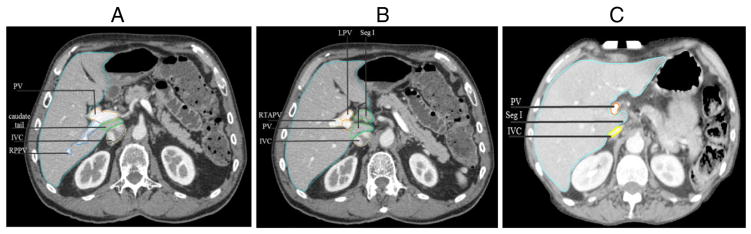
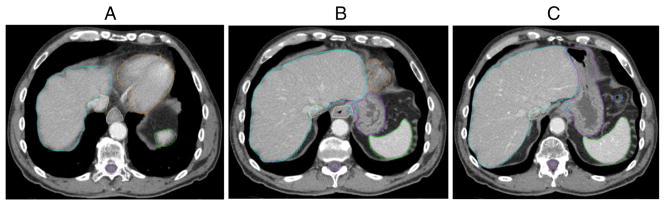
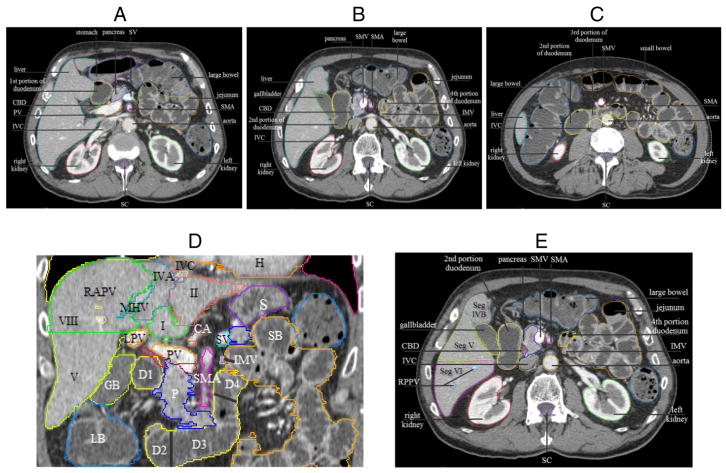
Methods and materials: Twelve expert radiation oncologists contoured the liver, esophagus, gastroesophageal junction (GEJ), stomach, duodenum, and common bile duct (CBD), and reviewed and edited 33 additional normal organ and blood vessel contours on an anonymized patient computed tomography (CT) dataset. Contours were overlaid and compared for agreement using MATLAB (MathWorks, Natick, MA). S95 contours, defined as the binomial distribution to generate 95% group consensus contours, and normal organ contouring definitions were generated and reviewed by the panel.
Results: There was excellent consistency and agreement of the liver, duodenal, and stomach contours, with substantial consistency for the esophagus contour, and moderate consistency for the GEJ and CBD contours using a Kappa statistic. Consensus definitions, detailed normal organ contouring recommendations and high-resolution images were developed.
Conclusions: Consensus contouring guidelines and a CT image atlas should improve contouring uniformity in radiation oncology clinical planning and RTOG trials.
Copyright © 2014 American Society for Radiation Oncology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: None.
Figures

References
-
- Deasy JO, Blanco AI, Clark VH. CERR: a computational environment for radiotherapy research. Med Phys. 2003;30:979–985. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
