

Cataplexy--clinical aspects, pathophysiology and management strategy
- PMID: 24890646
- PMCID: PMC8788644
- DOI: 10.1038/nrneurol.2014.97
Cataplexy--clinical aspects, pathophysiology and management strategy
Abstract
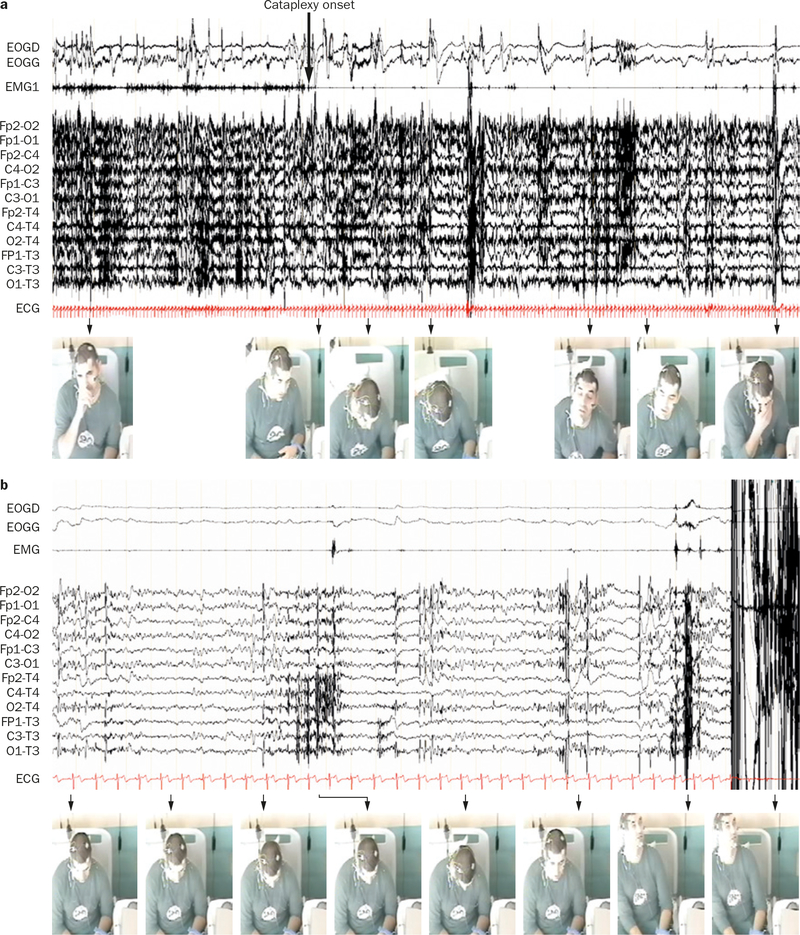
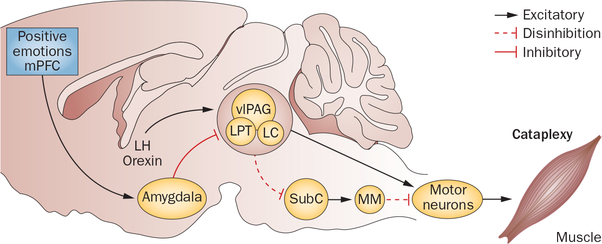
Cataplexy is the pathognomonic symptom of narcolepsy, and is the sudden uncontrollable onset of skeletal muscle paralysis or weakness during wakefulness. Cataplexy is incapacitating because it leaves the individual awake but temporarily either fully or partially paralyzed. Occurring spontaneously, cataplexy is typically triggered by strong positive emotions such as laughter and is often underdiagnosed owing to a variable disease course in terms of age of onset, presenting symptoms, triggers, frequency and intensity of attacks. This disorder occurs almost exclusively in patients with depletion of hypothalamic orexin neurons. One pathogenetic mechanism that has been hypothesized for cataplexy is the activation, during wakefulness, of brainstem circuitry that normally induces muscle tone suppression in rapid eye movement sleep. Muscle weakness during cataplexy is caused by decreased excitation of noradrenergic neurons and increased inhibition of skeletal motor neurons by γ-aminobutyric acid-releasing or glycinergic neurons. The amygdala and medial prefrontal cortex contain neural pathways through which positive emotions probably trigger cataplectic attacks. Despite major advances in understanding disease mechanisms in cataplexy, therapeutic management is largely symptomatic, with antidepressants and γ-hydroxybutyrate being the most effective treatments. This Review describes the clinical and pathophysiological aspects of cataplexy, and outlines optimal therapeutic management strategies.
Conflict of interest statement
Competing interests
Y.D. declares that he has received speaker honoraria and support for travel to meetings and has participated on the advisory boards for the following companies: UCB Pharma, JAZZ and Bioprojet. The other authors declare no competing interests.
Figures
References
-
- American Academy of Sleep Medicine. The international classification of sleep disorders, revised. Diagnostic and coding manual. European Society of Sleep Technology [online], http://www.esst.org/adds/ICSD.pdf (2001).
-
- Dauvilliers Y, Arnulf I & Mignot E Narcolepsy with cataplexy. Lancet 369, 499–511 (2007). - PubMed
-
- Overeem S, Mignot E, van Dijk JG & Lammers GJ Narcolepsy: clinical features, new pathophysiologic insights, and future perspectives. J. Clin. Neurophysiol. 18, 78–105 (2001). - PubMed
-
- Dauvilliers Y, Billiard M & Montplaisir J Clinical aspects and pathophysiology of narcolepsy. Clin. Neurophysiol. 114, 2000–2017 (2003). - PubMed
-
- Dauvilliers Y et al. Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology 57, 2029–2033 (2001). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
