

Evaluation of patient preference and willingness to pay for attributes of maintenance medication for chronic obstructive pulmonary disease (COPD)
- PMID: 24890711
- PMCID: PMC4240911
- DOI: 10.1007/s40271-014-0064-1
Evaluation of patient preference and willingness to pay for attributes of maintenance medication for chronic obstructive pulmonary disease (COPD)
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide. COPD is characterized by poor treatment adherence, and patient medication preferences may contribute to adherence.
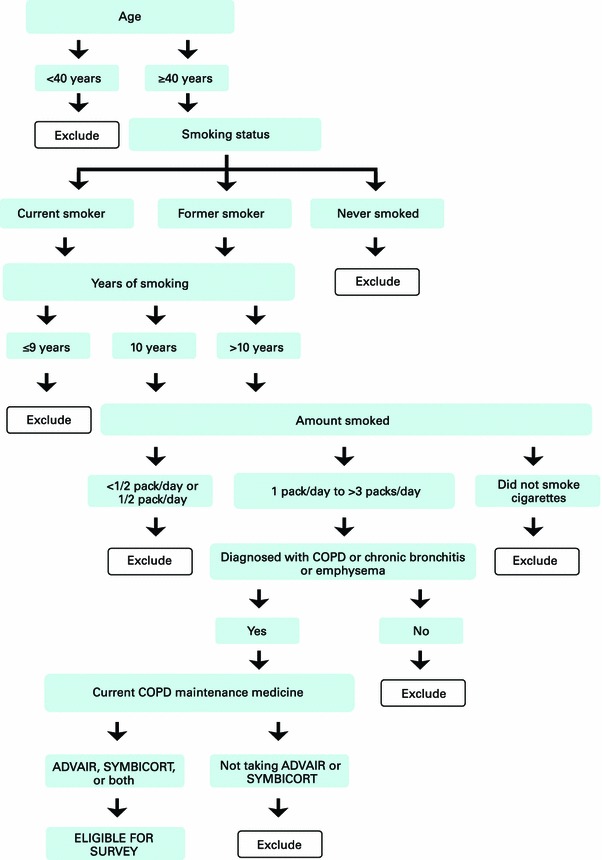
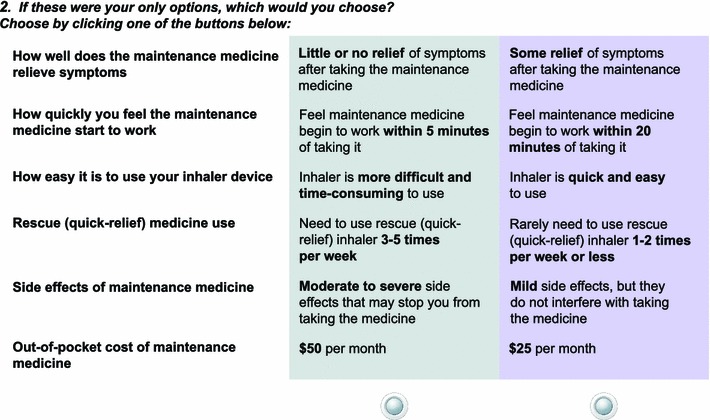
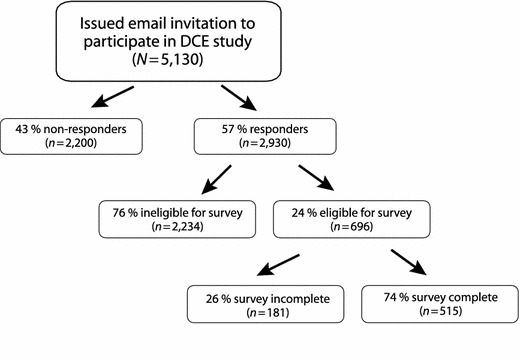
Methods: A discrete choice experiment with an internet panel drawn from the USA was used to evaluate preference and willingness to pay (WTP) of COPD patients for long-acting maintenance medications. Key attributes derived from earlier qualitative research (brief literature review and focus groups) with COPD patients on maintenance therapy included symptom relief, speed of feeling medication start to work, inhaler ease of use, rescue medication use, side effects, and monthly out-of-pocket co-pay. Patients were presented with hypothetical medications with different profiles and asked which they preferred. Utilities and marginal WTP in monthly co-pay dollars were estimated for all patients and by severity.
Results: Utilities for 515 participants were in the expected direction and highest for the most favorable attribute levels. Each attribute evaluated was important, and participants were willing to pay a premium to obtain each benefit. On average, WTP was as high as $US64 for complete symptom relief, $US59 for no side effects, $US32 to rarely use rescue medication, $US16 for a quick and easy to use inhaler, and $US13 for feeling medication work quickly (within 5 min; average WTP $US18/month for patients with severe/very severe COPD).
Conclusion: As expected, efficacy and safety were most valued by patients; however, this study showed that other COPD medication attributes, such as rescue medication, ease of use, and feeling medication work quickly, are also important in patient preferences.
Figures
References
-
- World Health Organization. Chronic obstructive pulmonary disease (COPD) burden; 2011. http://www.who.int/respiratory/copd/burden/en/index.html. Accessed March 2011.
-
- Mannino DM, Homa DM, Akinbami LJ, et al. Chronic obstructive pulmonary disease surveillance—United States, 1971–2000. MMWR Surveill Summ. 2002;51:1–16. - PubMed
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for diagnosis, management, and prevention of COPD. Revised 2011. http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-managem.... Accessed 1 June 2012.
-
- National Institute for Health and Clinical Excellence (NICE). Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care (update); 2010. http://guidance.nice.org.uk/CG101. Accessed 1 June 2012.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
