

Clinical characteristics and current treatment of glaucoma
- PMID: 24890835
- PMCID: PMC4031956
- DOI: 10.1101/cshperspect.a017236
Clinical characteristics and current treatment of glaucoma
Abstract
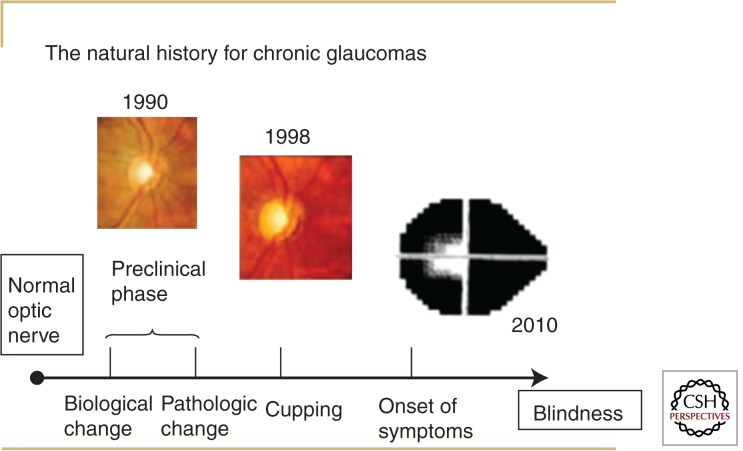
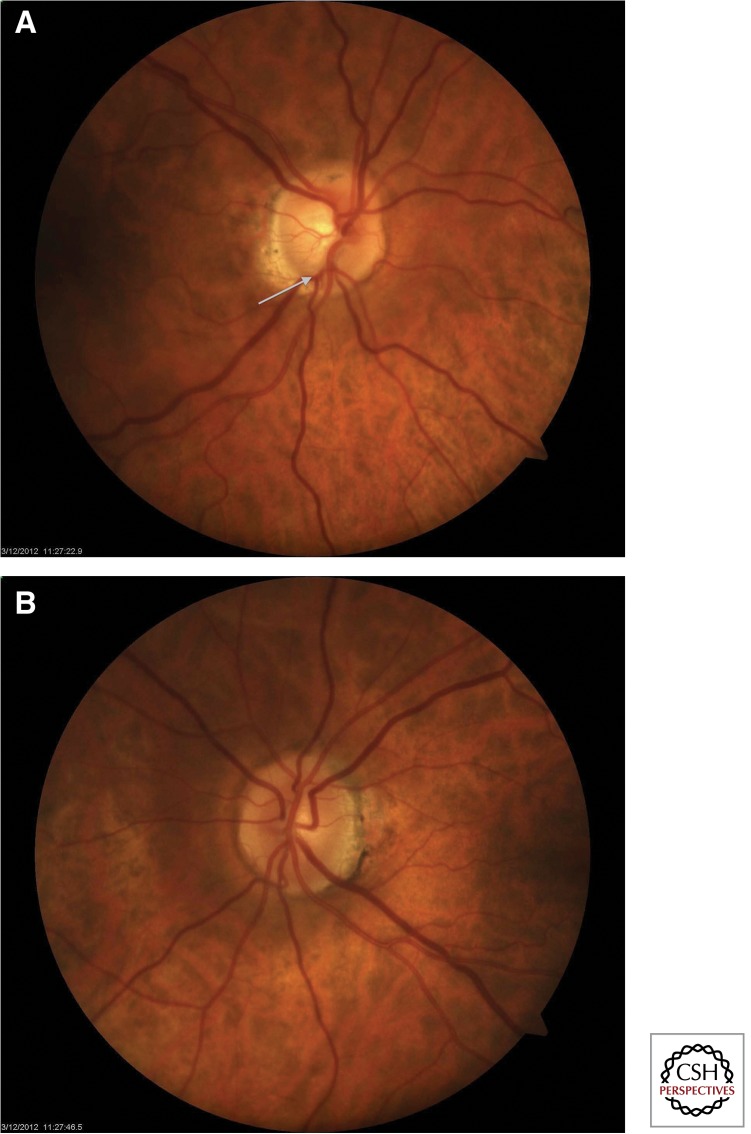
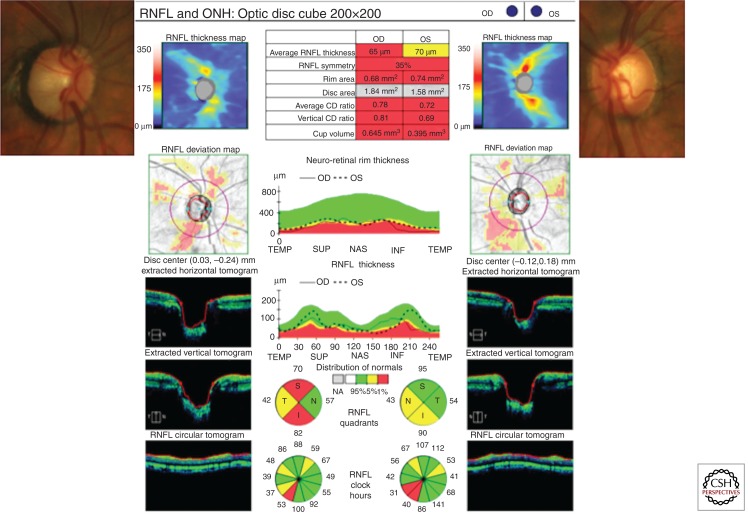
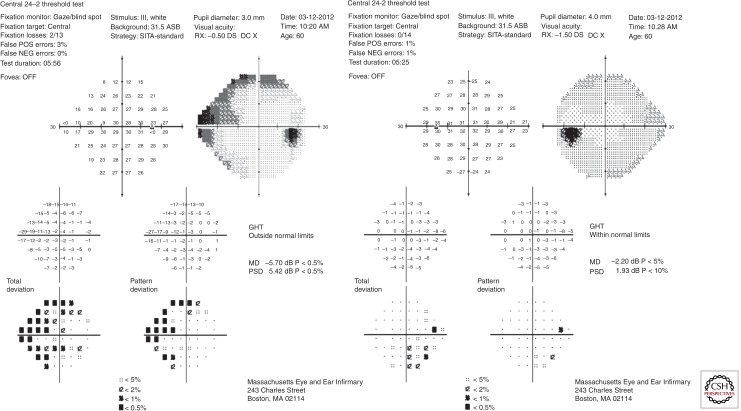
Glaucoma is a neurodegenerative disorder in which degenerating retinal ganglion cells (RGC) produce significant visual disability. Clinically, glaucoma refers to an array of conditions associated with variably elevated intraocular pressure (IOP) that contributes to RGC loss via mechanical stress, vascular abnormalities, and other mechanisms, such as immune phenomena. The clinical diagnosis of glaucoma requires assessment of the ocular anterior segment with slit lamp biomicroscopy, which allows the clinician to recognize signs of conditions that can produce elevated IOP. After measurement of IOP, a specialized prismatic lens called a gonioscope is used to determine whether the angle is physically open or closed. The structural manifestation of RGC loss is optic nerve head atrophy and excavation of the neuroretinal rim tissue. Treatment is guided by addressing secondary causes for elevated IOP (such as inflammation, infection, and ischemia) whenever possible. Subsequently, a variety of medical, laser, and surgical options are used to achieve a target IOP.
Copyright © 2014 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures
References
-
- Abe H, Hasegawa S, Iwata K 1987. Contrast sensitivity and pattern visual evoked potential in patients with glaucoma. Doc Ophthalmol 65: 65–70 - PubMed
-
- Aggarwal RK, Potamitis T, Chong NH, Guarro M, Shah P, Kheterpal S 1993. Extensive visual loss with topical facial steroids. Eye (Lond) 7: 664–666 - PubMed
-
- Anderson DR 2003. Collaborative normal tension glaucoma study. Curr Opin Ophthalmol 14: 86–90 - PubMed
-
- Bianchi-Marzoli S, Rizzo JF III, Brancato R, Lessell S 1995. Quantitative analysis of optic disc cupping in compressive optic neuropathy. Ophthalmology 102: 436–440 - PubMed
-
- Boland MV, Ervin AM, Friedman DS, Jampel HD, Hawkins BS, Vollenweider D, Chelladurai Y, Ward D, Suarez-Cuervo C, Robinson KA 2013. Comparative effectiveness of treatments for open-angle glaucoma: A systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 158: 271–279 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical