

Lichen planus: a clinical and immuno-histological analysis
- PMID: 24891656
- PMCID: PMC4037946
- DOI: 10.4103/0019-5154.131389
Lichen planus: a clinical and immuno-histological analysis
Abstract
Background: Direct immunofluorescence examination is an important technique in the diagnosis of cutaneous inflammatory disorders including lichen planus, especially in clinically and histopathological doubtful cases.
Objective: To study the diagnostic utility of intensity, number, and subtypes of positive immuno-reactants found in lichen planus.
Materials and methods: A detailed analysis of clinical as well as immuno-histological features of lichen planus cases was carried out.
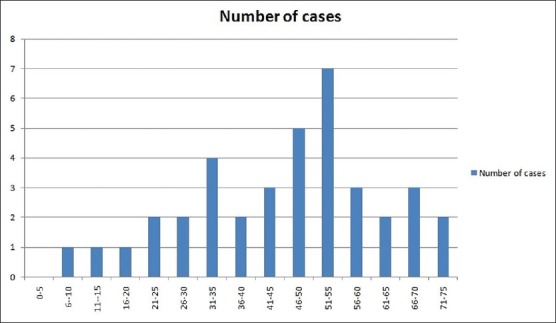
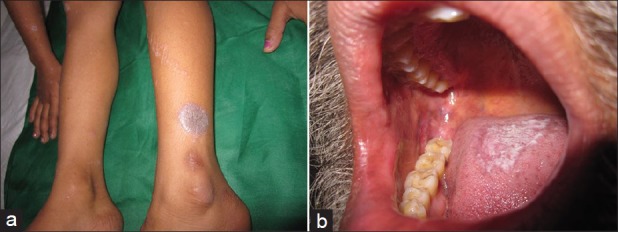
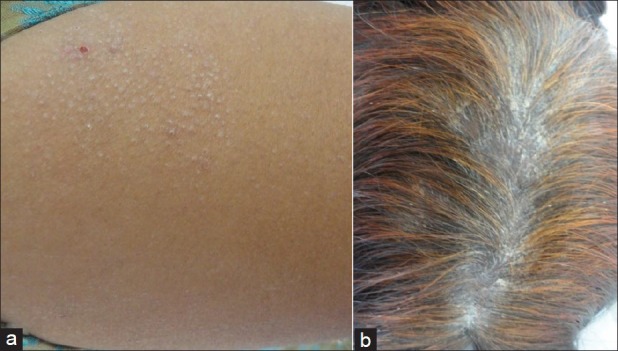
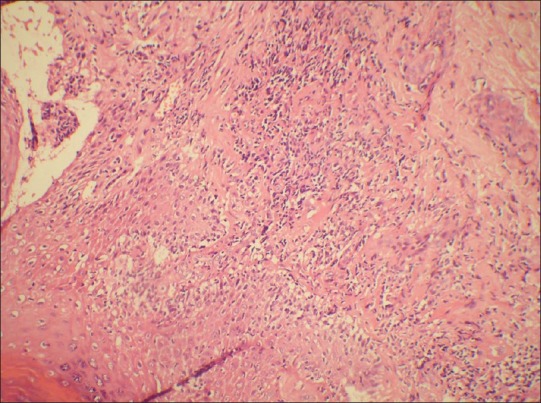
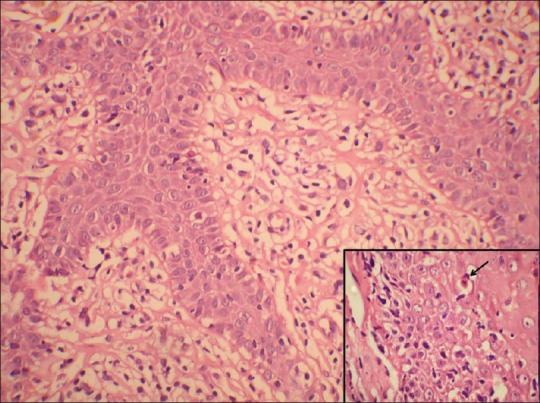
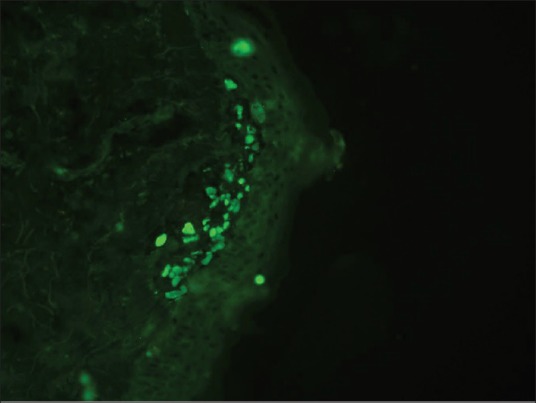
Results: The male to female ratio was 1:1.1. The largest number of patients was in 31-50 year age group. Itching was the most common presenting symptom. Papular lesions were seen in 53% cases. Remaining had hypertrophic (6), follicular (3) and mucosal (9) variants. Clinico-pathological discrepancies were observed in 3 patients. The characteristic histopathological changes including basal cell vacuolization, band-like lymphocytic infiltrate at dermo-epidermal junction were seen in all the biopsies while Civatte bodies were detected in 29% cases. The overall positive yield of direct immunofluorescence microscopy was 55%. Immune deposits at Civatte bodies and dermo-epidermal junction were detected in 47% and 8% of cases, respectively. Immunoglobulin M was the most common immunoreactant followed by immunoglobulin G.
Conclusions: There was no correlation found between the number and intensity of Civatte bodies with clinical variants of disease and also between the number of positive immunoreactants and clinical severity of the disease. The frequency, number, and arrangement of Civatte bodies in clusters in the papillary dermis as well as multiple immunoglobulins deposition at the Civatte bodies on direct immunofluorescence of skin biopsies are important features distinguishing lichen planus from other interface dermatitis.
Keywords: Direct immunofluorescence; interface dermatitis; skin biopsy.
Conflict of interest statement
Figures
References
-
- Mobini N, Toussaint S, Kamino H. Noninfectious erythematous, papular, and squamous siseases. In: Elder DE, Elenitsas R, Johnson BL, Murphy GF, editors. Lever's histopathology of the skin. 9th ed. Philadelphia: Lippincott Williams and Wilkins; 2005. pp. 180–214.
-
- Ellis FA. Histopathology of lichen planus based on analysis of one hundred biopsies. J Invest Dermatol. 1967;48:143–8. - PubMed
-
- Mutism DF, Adam BB. Immunofluorescence in dermatology. J Am Acad Dermatol. 2001;45:803–21. - PubMed
-
- Van der Meij EH, Schepman KP, Smeele LE, Van der Wal JE, Bezemer PD, Van der Waal I. A review of the recent literature regarding malignant transformation of oral lichen planus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:307–10. - PubMed
-
- Singh OP, Kanwar AJ. Lichen planus in India-an appraisal of 441 cases. Int J Dermatol. 1976;15:752–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources