

Diagnostic accuracy in detecting tears in the proximal biceps tendon using standard nonenhancing shoulder MRI
- PMID: 24891814
- PMCID: PMC4011903
- DOI: 10.2147/OAJSM.S58225
Diagnostic accuracy in detecting tears in the proximal biceps tendon using standard nonenhancing shoulder MRI
Abstract
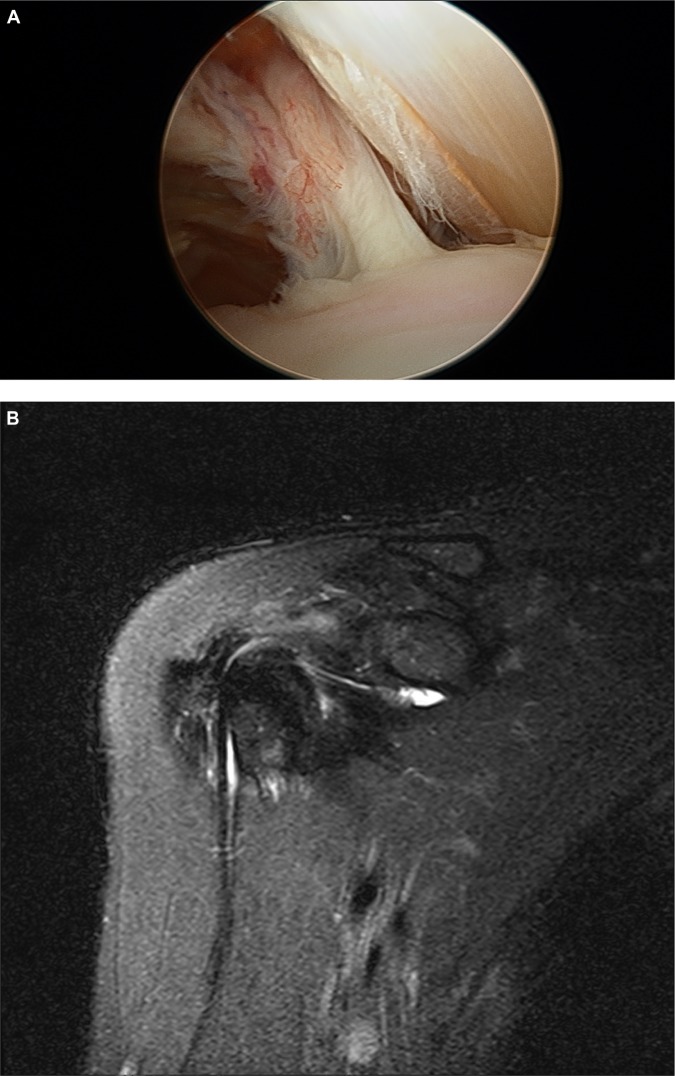
Background: There is a paucity of data in the literature evaluating the performance of noncontrast MRI in the diagnosis of partial and complete tears of the proximal portion of the long head of the biceps (LHB) tendon. The objective of this study was to evaluate the accuracy of noncontrast magnetic resonance imaging (MRI) compared to arthroscopy for the diagnosis of pathology involving the intra-articular portion of the LHB tendon.
Methods: We conducted a retrospective review of 66 patients (mean age 57.8 years, range 43-70 years) who underwent shoulder arthroscopy and evaluation of the LHB tendon after having had a noncontrast MRI of the shoulder. Biceps pathology was classified by both MRI and direct arthroscopic visualization as either normal, partial tearing, or complete rupture, and arthroscopy was considered to be the gold standard. We then determined the sensitivity, specificity, and positive- and negative-predictive values of MRI for the detection of partial and complete LHB tears.
Results: MRI identified 29/66 (43.9%) of patients as having a pathologic lesion of the LHB tendon (19 partial and ten complete tears) while diagnostic arthroscopy identified tears in 59/66 patients (89.4%; 50 partial and 16 complete). The sensitivity and specificity of MRI for detecting partial tearing of the LHB were 27.7% and 84.2%, respectively (positive predictive value =81.2%, negative predictive value =32.0%). The sensitivity and specificity of MRI for complete tears of the LHB were 56.3% and 98.0%, respectively (positive predictive value =90.0%, negative predictive value =87.5%).
Conclusion: Standard noncontrast MRI of the shoulder is limited in detecting partial tears and complete ruptures of the intra-articular LHB tendon. Surgeons may encounter pathologic lesions of the LHB tendon during arthroscopy that are not visualized on preoperative MRI.
Keywords: MRI detection; biceps tendon tear; case series; long head biceps tendon; magnetic resonance imaging.
Figures
Similar articles
-
Accuracy of MRI in diagnosing intra-articular pathology of the long head of the biceps tendon: results with a large cohort of patients.BMC Musculoskelet Disord. 2019 Jun 1;20(1):270. doi: 10.1186/s12891-019-2654-5. BMC Musculoskelet Disord. 2019. PMID: 31153372 Free PMC article.
-
Effect of patient age on accuracy of primary MRI signs of long head of biceps tearing and instability in the shoulder: an MRI-arthroscopy correlation study.Skeletal Radiol. 2018 Feb;47(2):203-214. doi: 10.1007/s00256-017-2783-6. Epub 2017 Oct 6. Skeletal Radiol. 2018. PMID: 28983764
-
Diagnostic performance of long head of biceps tendon tears on MRI: systematic review and meta-analysis.Eur Radiol. 2024 Jul;34(7):4309-4320. doi: 10.1007/s00330-023-10521-6. Epub 2023 Dec 27. Eur Radiol. 2024. PMID: 38148406
-
CT arthrography of the intra-articular long head of biceps tendon: Diagnostic performance outside the labral-bicipital complex.Diagn Interv Imaging. 2019 Jul-Aug;100(7-8):437-444. doi: 10.1016/j.diii.2019.02.005. Epub 2019 Mar 8. Diagn Interv Imaging. 2019. PMID: 30853414
-
Variations of the intra-articular portion of the long head of the biceps tendon: a classification of embryologically explained variations.J Shoulder Elbow Surg. 2009 Jul-Aug;18(4):556-65. doi: 10.1016/j.jse.2009.03.006. J Shoulder Elbow Surg. 2009. PMID: 19559371 Review.
Cited by
-
Long head of the biceps brachii tendon: unenhanced MRI versus direct MR arthrography.Skeletal Radiol. 2015 Sep;44(9):1263-72. doi: 10.1007/s00256-015-2152-2. Epub 2015 Apr 29. Skeletal Radiol. 2015. PMID: 25920387
-
Accuracy of MRI in diagnosing intra-articular pathology of the long head of the biceps tendon: results with a large cohort of patients.BMC Musculoskelet Disord. 2019 Jun 1;20(1):270. doi: 10.1186/s12891-019-2654-5. BMC Musculoskelet Disord. 2019. PMID: 31153372 Free PMC article.
-
Effect of patient age on accuracy of primary MRI signs of long head of biceps tearing and instability in the shoulder: an MRI-arthroscopy correlation study.Skeletal Radiol. 2018 Feb;47(2):203-214. doi: 10.1007/s00256-017-2783-6. Epub 2017 Oct 6. Skeletal Radiol. 2018. PMID: 28983764
-
A preliminary attempt to use radiomic features in the diagnosis of extra-articular long head biceps tendinitis.MAGMA. 2023 Aug;36(4):651-658. doi: 10.1007/s10334-022-01050-2. Epub 2022 Nov 30. MAGMA. 2023. PMID: 36449124
-
Diagnostic performance of long head of biceps tendon tears on MRI: systematic review and meta-analysis.Eur Radiol. 2024 Jul;34(7):4309-4320. doi: 10.1007/s00330-023-10521-6. Epub 2023 Dec 27. Eur Radiol. 2024. PMID: 38148406
References
-
- Alpantaki K, McLaughlin D, Karagogeos D, Hadjipavlou A, Kontakis G. Sympathetic and sensory neural elements in the tendon of the long head of the biceps. J Bone Joint Surg Am. 2005;87(7):1580–1583. - PubMed
-
- Elser F, Braun S, Dewing CB, Giphart JE, Millett PJ. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. 2011;27(4):581–592. - PubMed
-
- Longo UG, Loppini M, Marineo G, Khan WS, Maffulli N, Denaro V. Tendinopathy of the tendon of the long head of the biceps. Sports Med Arthrosc. 2011;19(4):321–332. - PubMed
-
- Nho SJ, Strauss EJ, Lenart BA, et al. Long head of the biceps tendinopathy: diagnosis and management. J Am Acad Orthop Surg. 2010;18(11):645–656. - PubMed
-
- Abboud JA, Bartolozzi AR, Widmer BJ, DeMola PM. Bicipital groove morphology on MRI has no correlation to intra-articular biceps tendon pathology. J Shoulder Elbow Surg. 2010;19(6):790–794. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
