

Microgravity environment and compensatory: Decompensatory phases for intracranial hypertension form new perspectives to explain mechanism underlying communicating hydrocephalus and its related disorders
- PMID: 24891884
- PMCID: PMC4038869
- DOI: 10.4103/1793-5482.131058
Microgravity environment and compensatory: Decompensatory phases for intracranial hypertension form new perspectives to explain mechanism underlying communicating hydrocephalus and its related disorders
Abstract
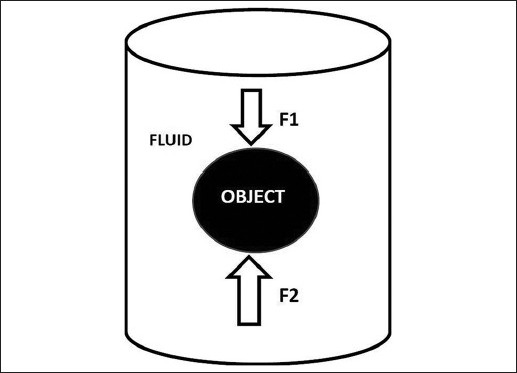
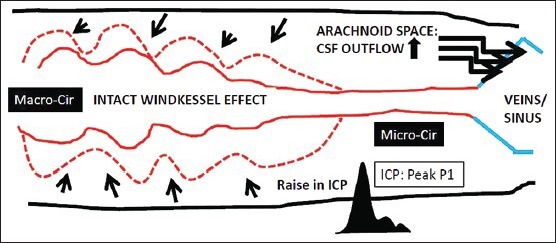
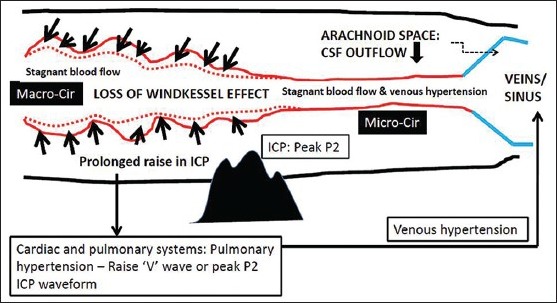
The pathogenesis underlying communicating hydrocephalus has been centered on impaired cerebrospinal fluid (CSF) outflow secondary to abnormal CSF pulsation and venous hypertension. Hydrodynamic theory of hydrocephalus fares better than traditional theory in explaining the possible mechanisms underlying communicating hydrocephalus. Nonetheless, hydrodynamic theory alone could not fully explain some conditions that have ventriculomegaly but without hydrocephalus. By revisiting brain buoyancy from a fresher perspective, called microgravity environment of the brain, introducing wider concepts of anatomical and physiological compensatory-decompensatory phases for a persistent raise in intracranial pressure, and along with combining these two concepts with the previously well-accepted concepts of Monro-Kellie doctrine, intracranial hypertension, cerebral blood flow, cerebral perfusion pressure, brain compliance and elasticity, cerebral autoregulation, blood-brain and blood-CSF barriers, venous and cardiopulmonary hypertension, Windkessel phenomenon, and cerebral pulsation, we provide plausible explanations to the pathogenesis for communicating hydrocephalus and its related disorders.
Keywords: Brain compliance; Monro – Kellie doctrine; Windkessel effect; brain pulsation; buoyancy; communicating hydrocephalus; microgravity.
Conflict of interest statement
Figures

References
-
- Egnor M, Zheng L, Rosiello A, Gutman F, Davis R. A model of pulsations in communicating hydrocephalus. Pediatr Neurosurg. 2002;36:281–303. - PubMed
-
- Greitz D. Radiological assessment of hydrocephalus: New theories and implications for therapy. Neurosurg Rev. 2004;27:145–65. - PubMed
-
- Czosnyka M, Smielewski P, Kirkpatrick P, Laing RJ, Menon D, Pickard JD. Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery. 1997;41:11–7. - PubMed
-
- Marshall I, MacCormick I, Sellar R, Whittle I. Assessment of factors affecting MRI measurement of intracranial volume changes and elastance index. Br J Neurosurg. 2008;22:389–97. - PubMed
-
- Portella G, Cormio M, Citerio G, Contant C, Kiening K, Enblad P, et al. Continuous cerebral compliance monitoring in severe head injury: Its relationship with intracranial pressure and cerebral perfusion pressure. Acta Neurochir (Wien) 2005;147:707–13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources