

Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth
- PMID: 24891990
- PMCID: PMC4030608
- DOI: 10.7453/gahmj.2014.019
Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth
Abstract
Objective: Patients with small intestine bacterial overgrowth (SIBO) have chronic intestinal and extraintestinal symptomatology which adversely affects their quality of life. Present treatment of SIBO is limited to oral antibiotics with variable success. A growing number of patients are interested in using complementary and alternative therapies for their gastrointestinal health. The objective was to determine the remission rate of SIBO using either the antibiotic rifaximin or herbals in a tertiary care referral gastroenterology practice.
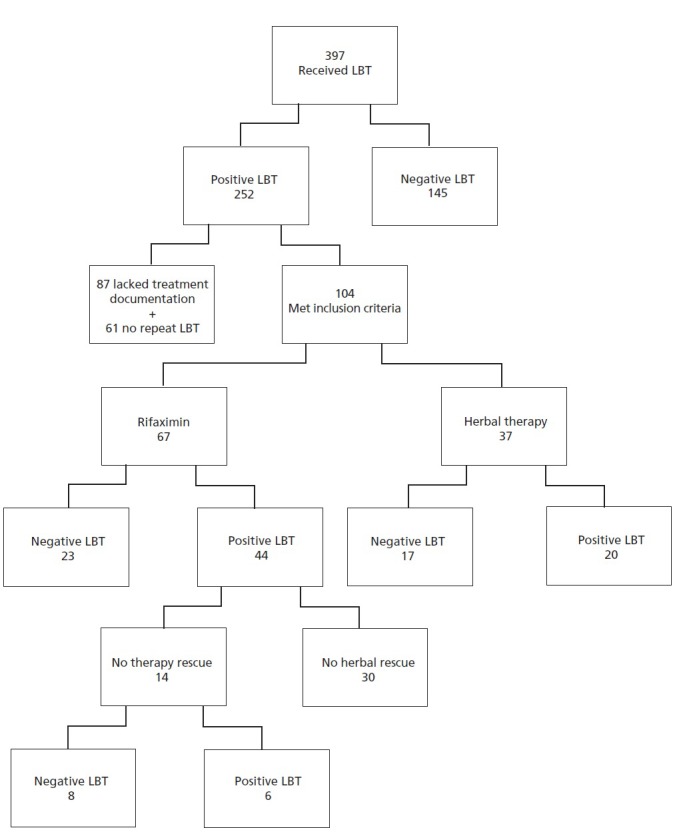
Design: One hundred and four patients who tested positive for newly diagnosed SIBO by lactulose breath testing (LBT) were offered either rifaximin 1200 mg daily vs herbal therapy for 4 weeks with repeat LBT post-treatment.
Results: Three hundred ninety-six patients underwent LBT for suspected SIBO, of which 251 (63.4%) were positive 165 underwent treatment and 104 had a follow-up LBT. Of the 37 patients who received herbal therapy, 17 (46%) had a negative follow-up LBT compared to 23/67 (34%) of rifaximin users (P=.24). The odds ratio of having a negative LBT after taking herbal therapy as compared to rifaximin was 1.85 (CI=0.77-4.41, P=.17) once adjusted for age, gender, SIBO risk factors and IBS status. Fourteen of the 44 (31.8%) rifaximin non-responders were offered herbal rescue therapy, with 8 of the 14 (57.1%) having a negative LBT after completing the rescue herbal therapy, while 10 non-responders were offered triple antibiotics with 6 responding (60%, P=.89). Adverse effects were reported among the rifaximin treated arm including 1 case of anaphylaxis, 2 cases of hives, 2 cases of diarrhea and 1 case of Clostridium difficile. Only one case of diarrhea was reported in the herbal therapy arm, which did not reach statistical significance (P=.22).
Conclusion: SIBO is widely prevalent in a tertiary referral gastroenterology practice. Herbal therapies are at least as effective as rifaximin for resolution of SIBO by LBT. Herbals also appear to be as effective as triple antibiotic therapy for SIBO rescue therapy for rifaximin non-responders. Further, prospective studies are needed to validate these findings and explore additional alternative therapies in patients with refractory SIBO.
Keywords: Antibiotics; Complementary and Alternative Medicine (CAM); Dysbiosis; Herbal Therapies; Irritable bowel syndrome (IBS); Small Intestine Bacterial Overgrowth (SIBO); rifaximin.
Figures
References
-
- Ford AC, Spiegel BM, Talley NJ, Moayyedi P. Small intestinal bacterial overgrowth in irritable bowel syndrome: systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2009;7(12):1279–86 - PubMed
-
- Choung RS, Ruff KC, Malhotra A, et al.Clinical predictors of small intestinal bacterial overgrowth by duodenal aspirate culture. Aliment Pharmacol Ther. 2011;33(9):1059–67 - PubMed
-
- Bohm M, Siwiec RM, Wo JM. Diagnosis and management of small intestinal bacterial overgrowth. Nutr Clin Pract. 2013;28(3):289–99 - PubMed
-
- Batt RM. Exocrine pancreatic insufficiency. Vet Clin North Am Small Anim Pract. 1993;23(3):595–608 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
