

Metabolic theory of septic shock
- PMID: 24892019
- PMCID: PMC4038812
- DOI: 10.5492/wjccm.v3.i2.45
Metabolic theory of septic shock
Abstract
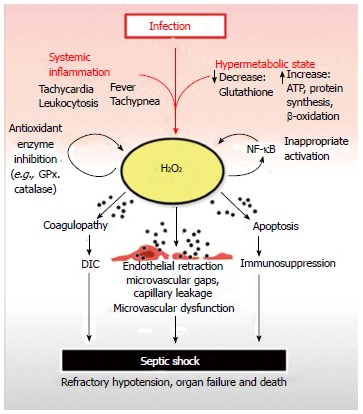
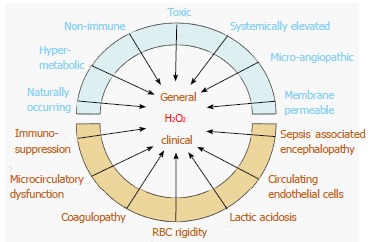
Septic shock is a life threatening condition that can develop subsequent to infection. Mortality can reach as high as 80% with over 150000 deaths yearly in the United States alone. Septic shock causes progressive failure of vital homeostatic mechanisms culminating in immunosuppression, coagulopathy and microvascular dysfunction which can lead to refractory hypotension, organ failure and death. The hypermetabolic response that accompanies a systemic inflammatory reaction places high demands upon stored nutritional resources. A crucial element that can become depleted early during the progression to septic shock is glutathione. Glutathione is chiefly responsible for supplying reducing equivalents to neutralize hydrogen peroxide, a toxic oxidizing agent that is produced during normal metabolism. Without glutathione, hydrogen peroxide can rise to toxic levels in tissues and blood where it can cause severe oxidative injury to organs and to the microvasculature. Continued exposure can result in microvascular dysfunction, capillary leakage and septic shock. It is the aim of this paper to present evidence that elevated systemic levels of hydrogen peroxide are present in septic shock victims and that it significantly contributes to the development and progression of this frequently lethal condition.
Keywords: Hydrogen peroxide; Hypermetabolic; Sepsis; Septic shock; Systemic inflammatory response syndrome.
Figures
Similar articles
-
Sepsis Care Pathway 2019.Qatar Med J. 2019 Nov 7;2019(2):4. doi: 10.5339/qmj.2019.qccc.4. eCollection 2019. Qatar Med J. 2019. PMID: 31763206 Free PMC article.
-
Sepsis: Evidence-based pathogenesis and treatment.World J Crit Care Med. 2021 Jul 9;10(4):66-80. doi: 10.5492/wjccm.v10.i4.66. eCollection 2021 Jul 9. World J Crit Care Med. 2021. PMID: 34316443 Free PMC article. Review.
-
Heartfelt sepsis: microvascular injury due to genomic storm.Kardiol Pol. 2018;76(8):1203-1216. doi: 10.5603/KP.a2018.0146. Epub 2018 Jul 5. Kardiol Pol. 2018. PMID: 29974447 Review.
-
The natural history of the systemic inflammatory response syndrome (SIRS). A prospective study.JAMA. 1995 Jan 11;273(2):117-23. JAMA. 1995. PMID: 7799491
-
Elevated nucleosome levels in systemic inflammation and sepsis.Crit Care Med. 2003 Jul;31(7):1947-51. doi: 10.1097/01.CCM.0000074719.40109.95. Crit Care Med. 2003. PMID: 12847387
Cited by
-
CD3D and CD247 are the molecular targets of septic shock.Medicine (Baltimore). 2023 Jul 21;102(29):e34295. doi: 10.1097/MD.0000000000034295. Medicine (Baltimore). 2023. PMID: 37478215 Free PMC article.
-
Hydrogen peroxide and disease: towards a unified system of pathogenesis and therapeutics.Mol Med. 2020 May 7;26(1):41. doi: 10.1186/s10020-020-00165-3. Mol Med. 2020. PMID: 32380940 Free PMC article. Review.
-
Effect of Hyperbaric Oxygen Therapy on Acute Liver Injury and Survival in a Rat Cecal Slurry Peritonitis Model.Life (Basel). 2020 Nov 15;10(11):283. doi: 10.3390/life10110283. Life (Basel). 2020. PMID: 33203111 Free PMC article.
-
Proteomic Approaches to Unravel Mechanisms of Antibiotic Resistance and Immune Evasion of Bacterial Pathogens.Front Med (Lausanne). 2022 May 2;9:850374. doi: 10.3389/fmed.2022.850374. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35586072 Free PMC article. Review.
-
A Metabolomics approach for the diagnosis Of SecondAry InfeCtions in COVID-19 (MOSAIC): a study protocol.BMC Infect Dis. 2021 Dec 2;21(1):1204. doi: 10.1186/s12879-021-06832-y. BMC Infect Dis. 2021. PMID: 34856937 Free PMC article.
References
-
- Goldenberg NM, Steinberg BE, Slutsky AS, Lee WL. Broken barriers: a new take on sepsis pathogenesis. Sci Transl Med. 2011;3:88ps25. - PubMed
-
- Marshall JC, Vincent JL, Guyatt G, Angus DC, Abraham E, Bernard G, Bombardier C, Calandra T, Jørgensen HS, Sylvester R, et al. Outcome measures for clinical research in sepsis: a report of the 2nd Cambridge Colloquium of the International Sepsis Forum. Crit Care Med. 2005;33:1708–1716. - PubMed
-
- American Cancer Society, Surveillance Research. Estimated New Cancer Cases and Deaths by Sex for All Sites, US, 2011. Available from: http://seer.cancer.gov/csr/1975_2008/results_single/sect_01_table.01.pdf....
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
