

Etanercept plus topical corticosteroids as initial therapy for grade one acute graft-versus-host disease after allogeneic hematopoietic cell transplantation
- PMID: 24892263
- PMCID: PMC4145722
- DOI: 10.1016/j.bbmt.2014.05.023
Etanercept plus topical corticosteroids as initial therapy for grade one acute graft-versus-host disease after allogeneic hematopoietic cell transplantation
Abstract
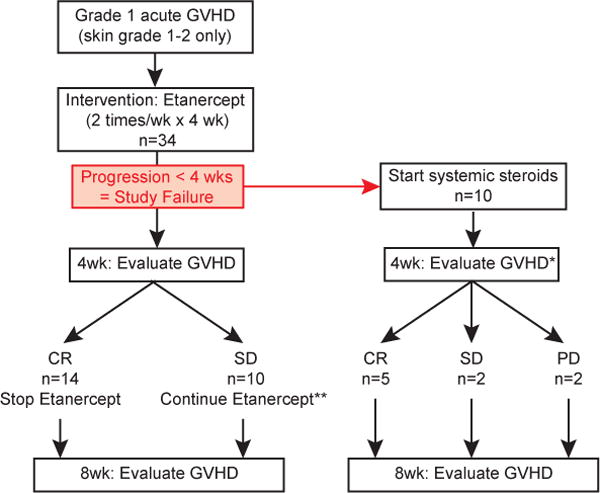
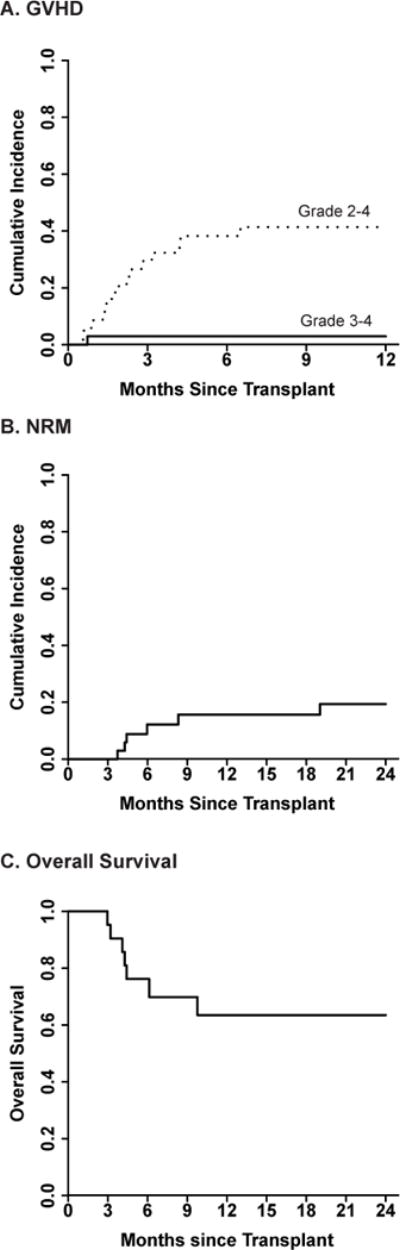
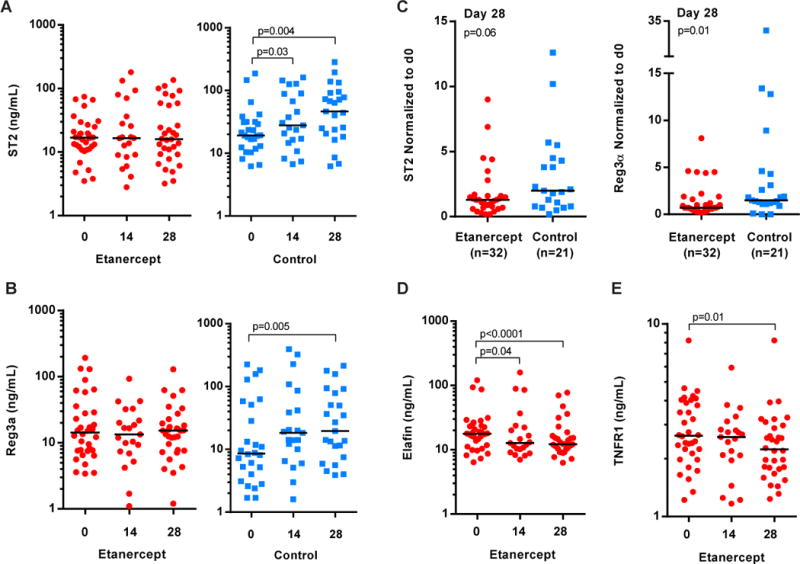
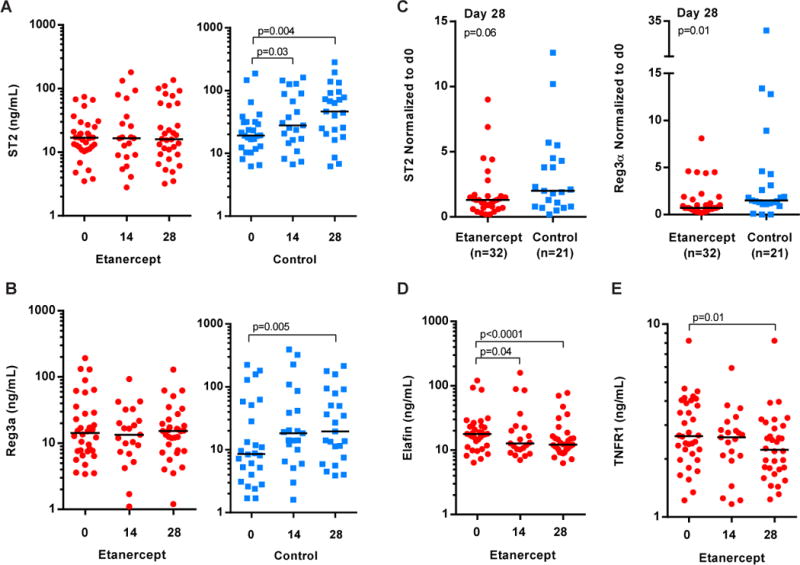
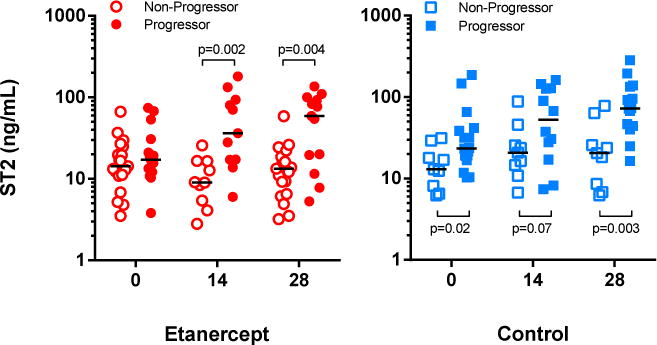
Clinical diagnosis of grade 1 acute graft-versus-host disease (GVHD) marks the beginning of a potentially progressive and fatal course of GVHD after hematopoietic stem cell transplantation (HSCT). However, interventional studies to treat early GVHD are lacking. We conducted a single-arm prospective phase II trial to test the hypothesis that treatment of newly diagnosed grade 1 acute GVHD with etanercept and topical corticosteroids would reduce progression to grade 2 to 4 within 28 days. Study patients (n = 34) had a median age of 51 years (range, 10 to 67 years) and had undergone unrelated (n = 22) or related (n = 12) donor HSCT. Study patients were treated with etanercept (.4 mg/kg, maximum 25 mg/dose) twice weekly for 4 to 8 weeks. Ten of 34 patients (29%) progressed to grade 2 to 4 acute GVHD within 28 days. The cumulative incidence of grade 2 to 4 and grade 3 to 4 acute GVHD at 1 year was 41% and 3%, respectively. Nonrelapse mortality was 19% and overall survival was 63% at 2 years. Among a contemporaneous control cohort of patients who were diagnosed with grade 1 acute GVHD and treated with topical corticosteroids but not etanercept during the study period, 12 of 28 patients (43%) progressed to grade 2 to 4 GVHD within 28 days, with a 1-year incidence of grade 2 to 4 GVHD and grade 3 to 4 GVHD of 61% (41% versus 61%, P = .08) and 18% (3% versus 18%, P = .05), respectively. Patients treated with etanercept also experienced less increase in GVHD plasma biomarkers suppression of tumorigenicity 2 (P = .06) and regenerating islet-derived 3-alpha (P = .01) 28 days after grade 1 acute GVHD diagnosis compared with contemporaneous control patients. This study was terminated early because of poor accrual. Future prospective studies are needed to identify patients with grade 1 acute GVHD at risk of swift progression to more severe GVHD and to establish consensus for the treatment of grade 1 acute GVHD. This trial is registered with ClinicalTrials.gov, number NCT00726375.
Keywords: Clinical trial; Etanercept; Grade 1 acute; Graft-versus-host disease; Hematopoietic stem cell transplantation.
Copyright © 2014 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Copelan EA. Hematopoietic stem-cell transplantation. The New England journal of medicine. 2006;354:1813–26. - PubMed
-
- Nash RA, Antin JH, Karanes C, Fay JW, Avalos BR, Yeager AM, et al. Phase 3 study comparing methotrexate and tacrolimus with methotrexate and cyclosporine for prophylaxis of acute graft-versus-host disease after marrow transplantation from unrelated donors. Blood. 2000;96:2062–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
