

Gastric cáncer: Overview
- PMID: 24892619
- PMCID: PMC4002033
Gastric cáncer: Overview
Abstract
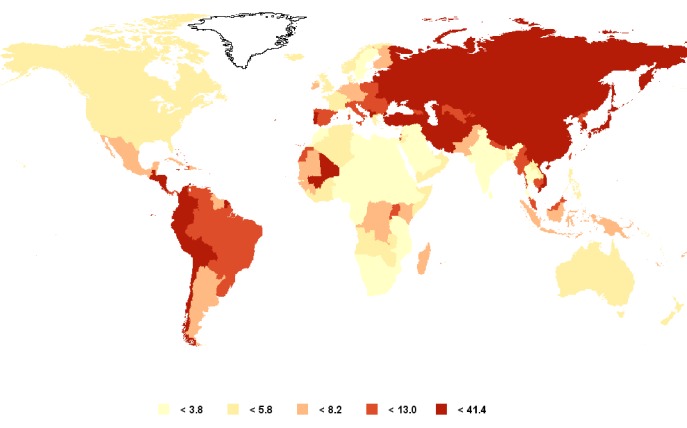
Gastric cancer ranks fourth in incidence and second in mortality among all cancers worldwide. Despite the decrease in incidence in some regions of the world, gastric cancer continues to present a major clinical challenge due to most cases being diagnosed in advanced stages with poor prognosis and limited treatment options. The development of gastric cancer is a complex and multifactorial process involving a number of etiological factors and multiple genetic and epigenetic alterations. Among the predisposing factors are: Helicobacter pylori infection, high salt intake, smoking, and in a small percentage of patients, a familial genetic component. More than 95% of stomach cancer cases are adenocarcinomas, which are classified into two major histologic types: intestinal and diffuse. Intestinal type adenocarcinoma is preceded by a sequence of gastric lesions known as Correa´s cascade and is the histologic type associated with the global decrease in gastric cancer rates. Diffuse type adenocarcinomas have a more aggressive behavior and worse prognosis than those of the intestinal type. According to the anatomical location, adenocarcinomas are classified as proximal (originating in the cardia) and distal (originating in the body and antrum). This classification seems to recognize two different clinical entities. Surgical resection of the tumor at an early stage is the only effective treatment method. Therefore, the identification and surveillance of patients at risk may play a significant role in survival rates. Anti-Helicobacter pylori therapy has been shown to be an effective measure in the prevention of gastric cancer.
El cáncer gástrico ocupa el cuarto lugar en incidencia y el segundo en mortalidad entre todos los cánceres en todo el mundo. A pesar de la disminución de la incidencia en algunas regiones del mundo, el cáncer gástrico continúa siendo un reto clínico debido a que la mayoría de los casos se diagnostican en etapas avanzadas con mal pronóstico y opciones de tratamiento limitadas. El desarrollo de cáncer gástrico es un proceso complejo y multifactorial que implica un número de factores etiológicos y múltiples alteraciones. Entre genética y epigenética los factores predisponentes son: infección por Helicobacter pylori, alto consumo de sal, fumar, y en un pequeño porcentaje de los pacientes, un componente genético familiar. Más del 95% de los casos de cáncer de estómago son adenocarcinomas, que se clasifican en dos principales tipos histológicos: intestinal y difuso. Adenocarcinomas de tipo intestinal están precedidos por una secuencia de lesiones gástricas conocidas como cascada de Correa y es el tipo histológico asociado con la disminución global de las tasas de cáncer gástrico. Adenocarcinomas de tipo difuso tienen un comportamiento más agresivo y peor pronóstico que aquellos del tipo intestinal. De acuerdo con la localización anatómica, los adenocarcinomas se clasifican como proximal (originario en el cardias) y distal (que se origina en el cuerpo y antro). Este clasificación parece reconocer dos entidades clínicas diferentes. La resección quirúrgica del tumor en estadios tempranos es el único método de tratamiento efectivo. Por lo tanto, la identificación y vigilancia de los pacientes en situación de riesgo pueden desempeñar un papel importante en las tasas de supervivencia. El tratamiento Anti-Helicobacter pylori ha demostrado ser una medida eficaz en la prevención del cáncer gástrico.
Keywords: Gastric cancer; Helicobacter pylori; dysplasia; epidemiology; gastric adenocarcinoma; intestinal metaplasia; multifocal atrophic gastritis.
Conflict of interest statement
Figures


References
-
- Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO Classification of tumours of the digestive system, 4th edition.Lyon, France: International Agency for Research on Cancer; 2010.
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide. France: International Agency for Research on Cancer; 2010.
-
- Lauwers GY, Shimizu M, Correa P, Forman D, Mathers C, Parkin DM. Evaluation of gastric biopsies for neoplasia: differences between Japanese and Western pathologists. Am J Surg Pathol. 1999;23:511–518. - PubMed
-
- Brown LM, Devesa SS. Epidemiologic trends in esophageal and gastric cancer in the United States. Surg Oncol Clin N Am. 2002;11:235–256. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
