

The inextricable role of the kidney in hypertension
- PMID: 24892708
- PMCID: PMC4092877
- DOI: 10.1172/JCI72274
The inextricable role of the kidney in hypertension
Abstract
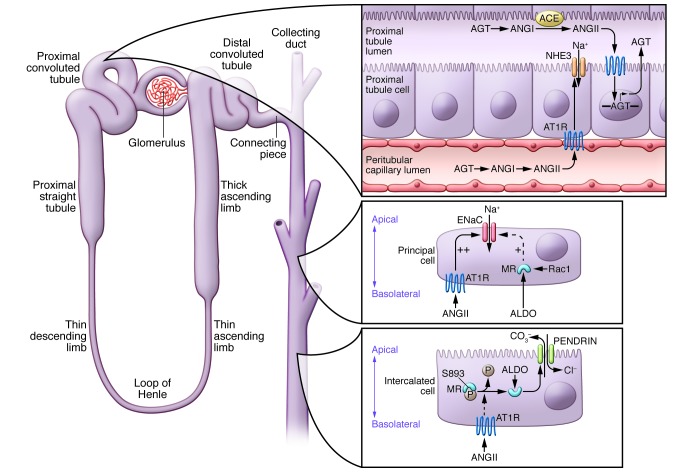
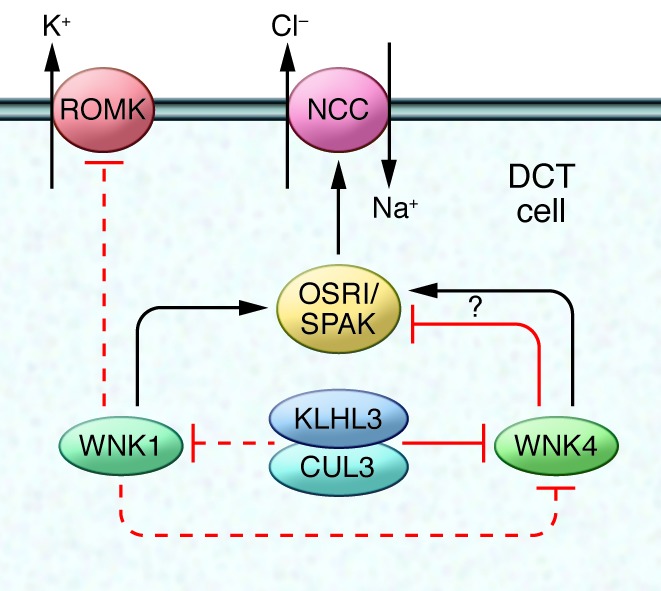
An essential link between the kidney and blood pressure control has long been known. Here, we review evidence supporting the premise that an impaired capacity of the kidney to excrete sodium in response to elevated blood pressure is a major contributor to hypertension, irrespective of the initiating cause. In this regard, recent work suggests that novel pathways controlling key sodium transporters in kidney epithelia have a critical impact on hypertension pathogenesis, supporting a model in which impaired renal sodium excretion is a final common pathway through which vascular, neural, and inflammatory responses raise blood pressure. We also address recent findings calling into question long-standing notions regarding the relationship between sodium intake and changes in body fluid volume. Expanded understanding of the role of the kidney as both a cause and target of hypertension highlights key aspects of pathophysiology and may lead to identification of new strategies for prevention and treatment.
Figures
References
-
- [No authors listed]. Effects of treatment on morbidity in hypertension. Results in patients with diastolic blood pressures averaging 115 through 129 mm Hg. JAMA. 1967202111028–1034. - PubMed
-
- [No authors listed]. Five-year findings of the hypertension detection follow-up program. I. Reduction in mortality of persons with high blood pressure, including mild hypertension. Hypertension Detection and Follow-up Program Cooperative Group. JAMA. 1979242232562–2571. - PubMed
-
- Gu Q, Burt VL, Dillon CF, Yoon S. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension: the National Health And Nutrition Examination Survey, 2001 to 2010. Circulation. 2012;126(17):2105–2114. doi: 10.1161/CIRCULATIONAHA.112.096156. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
