

Neurologic complications of bariatric surgery
- PMID: 24893235
- PMCID: PMC10564007
- DOI: 10.1212/01.CON.0000450967.76452.f2
Neurologic complications of bariatric surgery
Abstract
Purpose of review: The increasing utilization of bariatric surgery has been accompanied by an increased incidence and awareness of related neurologic complications. The purpose of this review is to provide up-to-date information on the neurologic complications related to bariatric surgery.
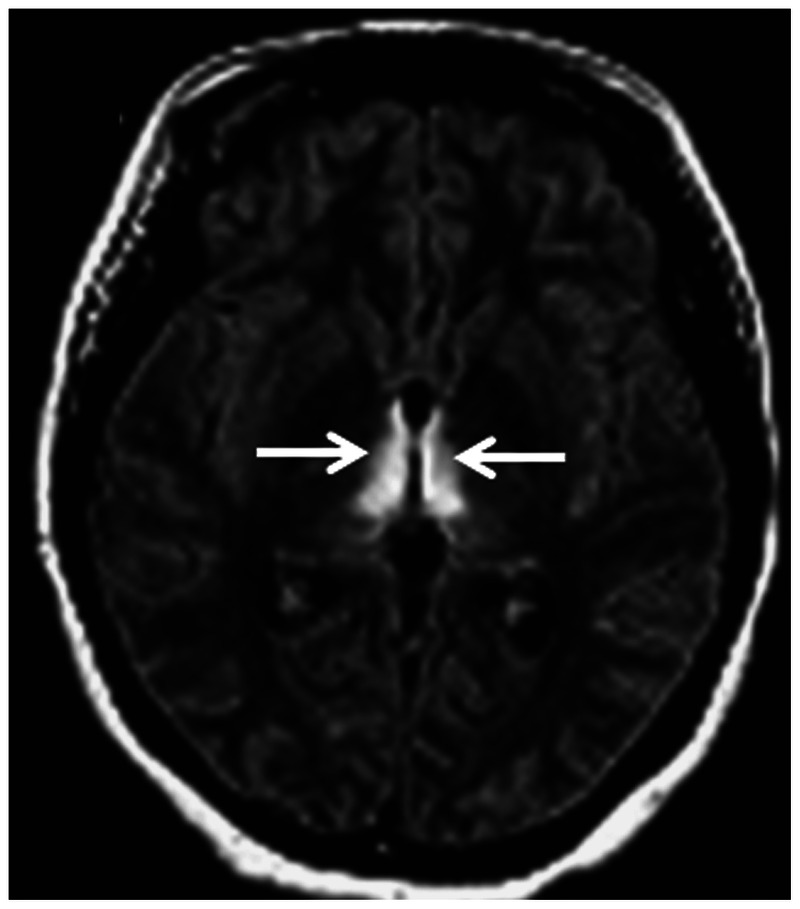
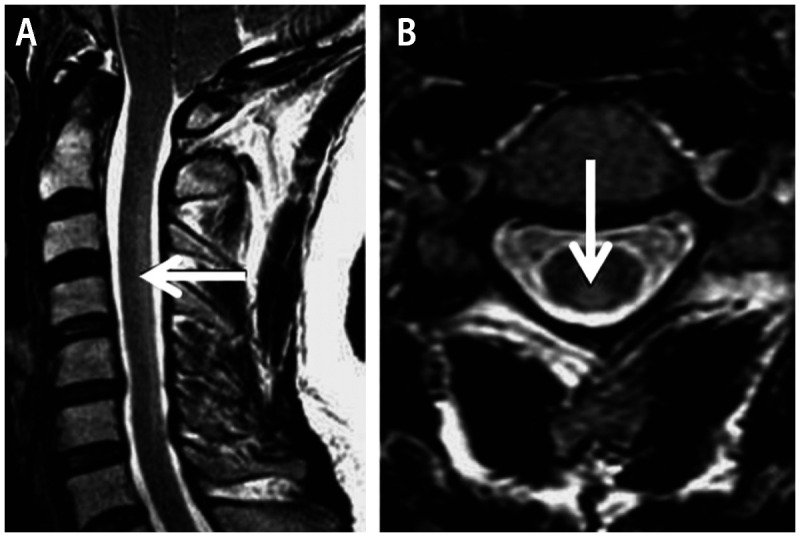
Recent findings: Neurologic complications related to bariatric surgery are predominantly due to nutrient deficiencies. Common early complications include Wernicke encephalopathy due to thiamine deficiency, and late complications include myelopathy or myeloneuropathy due to vitamin B12 or copper deficiency.
Summary: Early recognition and prompt institution of treatment is essential to prevent long-term disability. Often, life-long supplementation may be required.
Figures
References
-
- Mechanick JI,, Kushner RF,, Sugerman HJ, et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract 2008; 14 (suppl 1): 1–83. - PubMed
-
- Buchwald H. Metabolic surgery: a brief history and perspective. Surg Obes Relat Dis 2010; 6 (2): 221–222. - PubMed
-
- Mechanick JI,, Youdim A,, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Obesity (Silver Spring) 2013; 21 (suppl 1): S1–S27. - PMC - PubMed
-
- Abarbanel JM,, Berginer VM,, Osimani A, et al. Neurologic complications after gastric restriction surgery for morbid obesity. Neurology 1987; 37 (2): 196–200. - PubMed
-
- Berger JR. The neurological complications of bariatric surgery. Arch Neurol 2004; 61 (8): 1185–1189. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials