

The effectiveness of computerized order entry at reducing preventable adverse drug events and medication errors in hospital settings: a systematic review and meta-analysis
- PMID: 24894078
- PMCID: PMC4096499
- DOI: 10.1186/2046-4053-3-56
The effectiveness of computerized order entry at reducing preventable adverse drug events and medication errors in hospital settings: a systematic review and meta-analysis
Abstract
Background: The Health Information Technology for Economic and Clinical Health (HITECH) Act subsidizes implementation by hospitals of electronic health records with computerized provider order entry (CPOE), which may reduce patient injuries caused by medication errors (preventable adverse drug events, pADEs). Effects on pADEs have not been rigorously quantified, and effects on medication errors have been variable. The objectives of this analysis were to assess the effectiveness of CPOE at reducing pADEs in hospital-related settings, and examine reasons for heterogeneous effects on medication errors.
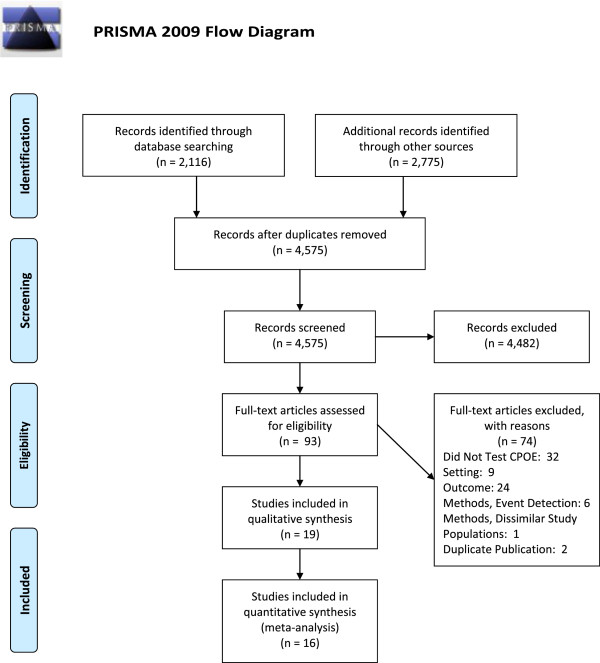
Methods: Articles were identified using MEDLINE, Cochrane Library, Econlit, web-based databases, and bibliographies of previous systematic reviews (September 2013). Eligible studies compared CPOE with paper-order entry in acute care hospitals, and examined diverse pADEs or medication errors. Studies on children or with limited event-detection methods were excluded. Two investigators extracted data on events and factors potentially associated with effectiveness. We used random effects models to pool data.
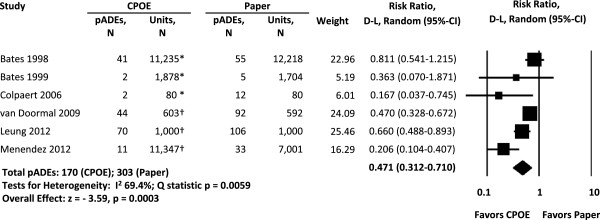
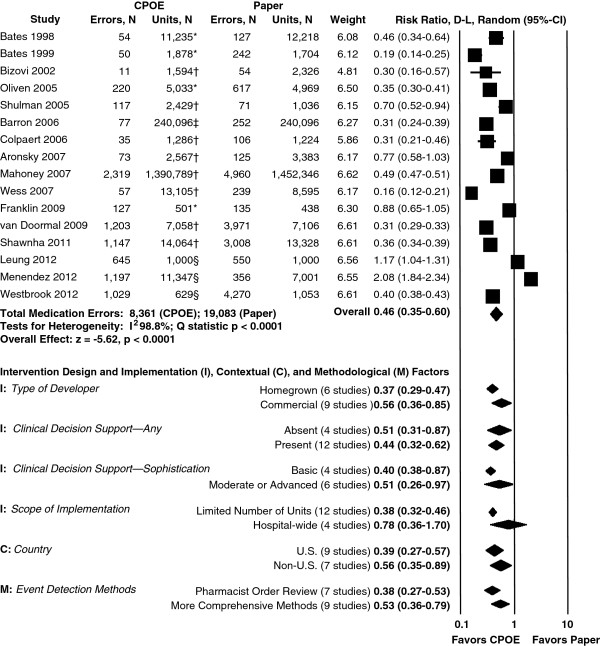
Results: Sixteen studies addressing medication errors met pooling criteria; six also addressed pADEs. Thirteen studies used pre-post designs. Compared with paper-order entry, CPOE was associated with half as many pADEs (pooled risk ratio (RR) = 0.47, 95% CI 0.31 to 0.71) and medication errors (RR = 0.46, 95% CI 0.35 to 0.60). Regarding reasons for heterogeneous effects on medication errors, five intervention factors and two contextual factors were sufficiently reported to support subgroup analyses or meta-regression. Differences between commercial versus homegrown systems, presence and sophistication of clinical decision support, hospital-wide versus limited implementation, and US versus non-US studies were not significant, nor was timing of publication. Higher baseline rates of medication errors predicted greater reductions (P < 0.001). Other context and implementation variables were seldom reported.
Conclusions: In hospital-related settings, implementing CPOE is associated with a greater than 50% decline in pADEs, although the studies used weak designs. Decreases in medication errors are similar and robust to variations in important aspects of intervention design and context. This suggests that CPOE implementation, as subsidized under the HITECH Act, may benefit public health. More detailed reporting of the context and process of implementation could shed light on factors associated with greater effectiveness.
Figures
References
-
- Blumenthal D. Wiring the health system–origins and provisions of a new federal program. N Engl J Med. 2011;365(24):2323–2329. - PubMed
-
- Classen DC, Bates DW. Finding the meaning in meaningful use. N Engl J Med. 2011;365(9):855–8. doi:10.1056/NEJMsb1103659. - PubMed
-
- Desroches CM, Charles D, Furukawa MF, Joshi MS, Kralovec P, Mostashari F, Worzala C, Jha AK. Adoption of electronic health records grows rapidly, but fewer than half of US hospitals had at least a basic system in 2012. Health Aff (Millwood) 2013;32(8):1478–1485. - PubMed
-
- Eslami S, de Keizer NF, Abu-Hanna A. The impact of computerized physician medication order entry in hospitalized patients–a systematic review. Int J Med Inform. 2008;77(6):365–376. - PubMed
-
- Weir CR, Staggers N, Phansalkar S. The state of the evidence for computerized provider order entry: a systematic review and analysis of the quality of the literature. Int J Med Inform. 2009;78(6):365–374. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
