

Advance distribution of misoprostol for prevention of postpartum hemorrhage (PPH) at home births in two districts of Liberia
- PMID: 24894566
- PMCID: PMC4055371
- DOI: 10.1186/1471-2393-14-189
Advance distribution of misoprostol for prevention of postpartum hemorrhage (PPH) at home births in two districts of Liberia
Abstract
Background: A postpartum hemorrhage prevention program to increase uterotonic coverage for home and facility births was introduced in two districts of Liberia. Advance distribution of misoprostol was offered during antenatal care (ANC) and home visits. Feasibility, acceptability, effectiveness of distribution mechanisms and uterotonic coverage were evaluated.
Methods: Eight facilities were strengthened to provide PPH prevention with oxytocin, PPH management and advance distribution of misoprostol during ANC. Trained traditional midwives (TTMs) as volunteer community health workers (CHWs) provided education to pregnant women, and district reproductive health supervisors (DRHSs) distributed misoprostol during home visits. Data were collected through facility and DRHS registers. Postpartum interviews were conducted with a sample of 550 women who received advance distribution of misoprostol on place of delivery, knowledge, misoprostol use, and satisfaction.
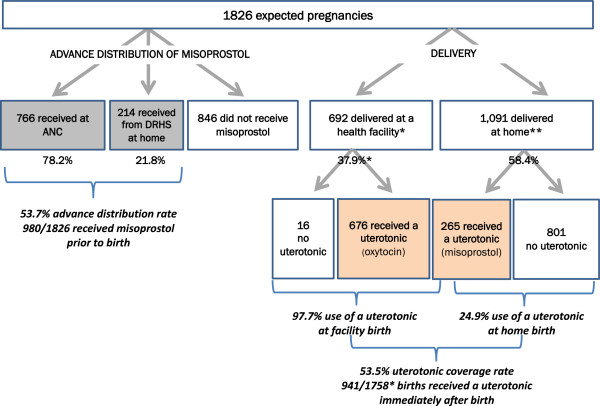
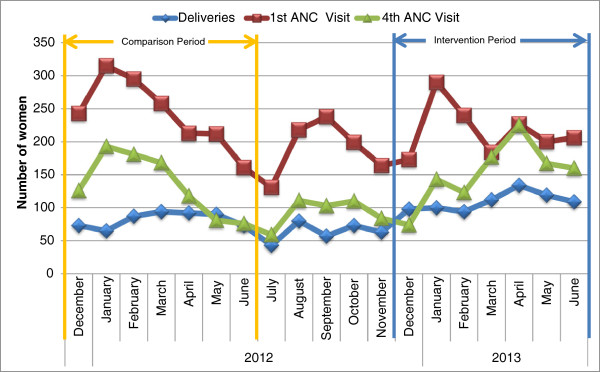
Results: There were 1826 estimated deliveries during the seven-month implementation period. A total of 980 women (53.7%) were enrolled and provided misoprostol, primarily through ANC (78.2%). Uterotonic coverage rate of all deliveries was 53.5%, based on 97.7% oxytocin use at recorded facility vaginal births and 24.9% misoprostol use at home births. Among 550 women interviewed postpartum, 87.7% of those who received misoprostol and had a home birth took the drug. Sixty-three percent (63.0%) took it at the correct time, and 54.0% experienced at least one minor side effect. No serious adverse events reported among enrolled women. Facility-based deliveries appeared to increase during the program.
Conclusions: The program was moderately effective at achieving high uterotonic coverage of all births. Coverage of home births was low despite the use of two channels of advance distribution of misoprostol. Although ANC reached a greater proportion of women in late pregnancy than home visits, 46.3% of expected deliveries did not receive education or advance distribution of misoprostol. A revised community-based strategy is needed to increase advance distribution rates and misoprostol coverage rates for home births. Misoprostol for PPH prevention appears acceptable to women in Liberia. Correct timing of misoprostol self-administration needs improved emphasis during counseling and education.
Figures
Similar articles
-
Misoprostol for postpartum hemorrhage prevention at home birth: an integrative review of global implementation experience to date.BMC Pregnancy Childbirth. 2013 Feb 20;13:44. doi: 10.1186/1471-2393-13-44. BMC Pregnancy Childbirth. 2013. PMID: 23421792 Free PMC article. Review.
-
Postpartum hemorrhage prevention in Nepal: a program assessment.BMC Pregnancy Childbirth. 2017 Jun 5;17(1):169. doi: 10.1186/s12884-017-1347-z. BMC Pregnancy Childbirth. 2017. PMID: 28583092 Free PMC article.
-
Advance distribution of misoprostol for the prevention of postpartum hemorrhage in South Sudan.Int J Gynaecol Obstet. 2014 Nov;127(2):183-8. doi: 10.1016/j.ijgo.2014.05.016. Epub 2014 Jul 9. Int J Gynaecol Obstet. 2014. PMID: 25051905
-
Increasing Access to Prevention of Postpartum Hemorrhage Interventions for Births in Health Facilities and at Home in Four Districts of Rwanda.Afr J Reprod Health. 2015 Dec;19(4):58-67. Afr J Reprod Health. 2015. PMID: 27337854
-
Advance misoprostol distribution to pregnant women for preventing and treating postpartum haemorrhage.Cochrane Database Syst Rev. 2020 Jun 23;6(6):CD009336. doi: 10.1002/14651858.CD009336.pub2. Cochrane Database Syst Rev. 2020. PMID: 35819305 Free PMC article. Review.
Cited by
-
Scaling up interventions: findings and lessons learned from an external evaluation of Niger's National Initiative to reduce postpartum hemorrhage.BMC Pregnancy Childbirth. 2019 Oct 24;19(1):379. doi: 10.1186/s12884-019-2502-5. BMC Pregnancy Childbirth. 2019. PMID: 31651264 Free PMC article.
-
Variation in maternal mortality in Sidama National Regional State, southern Ethiopia: A population based cross sectional household survey.PLoS One. 2023 Mar 7;18(3):e0272110. doi: 10.1371/journal.pone.0272110. eCollection 2023. PLoS One. 2023. PMID: 36881577 Free PMC article.
-
Prevention of postpartum haemorrhage by community-based auxiliary midwives in hard-to-reach areas of Myanmar: a qualitative inquiry into acceptability and feasibility of task shifting.BMC Pregnancy Childbirth. 2017 May 17;17(1):146. doi: 10.1186/s12884-017-1324-6. BMC Pregnancy Childbirth. 2017. PMID: 28514959 Free PMC article.
-
The Safety and Feasibility of a Family First Aid Approach for the Management of Postpartum Hemorrhage in Home Births: A Pre-post Intervention Study in Rural Pakistan.Matern Child Health J. 2021 Jan;25(1):118-126. doi: 10.1007/s10995-020-03047-6. Epub 2020 Nov 26. Matern Child Health J. 2021. PMID: 33242210 Free PMC article.
-
Factors influencing rapid progress in child health in post-conflict Liberia: a mixed methods country case study on progress in child survival, 2000-2013.BMJ Open. 2018 Oct 15;8(10):e021879. doi: 10.1136/bmjopen-2018-021879. BMJ Open. 2018. PMID: 30327401 Free PMC article.
References
-
- World Health Organization. Trends in Maternal Mortality: 1990 to 2008. World Health Organization; 2010. http://whqlibdoc.who.int/publications/2010/9789241500265_eng.pdf.
-
- Liberia Institute of Statistics and Geo-Information Services (LISGIS) [Liberia], Ministry of Health and Social Welfare [Liberia], National AIDS Control Program [Liberia], and Macro International Inc. Liberia Demographic and Health Survey. 2007. http://dhsprogram.com/pubs/pdf/FR201/FR201.pdf.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
