

Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in patients with gynaecological malignancies
- PMID: 24894643
- PMCID: PMC6457854
- DOI: 10.1002/14651858.CD007387.pub3
Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in patients with gynaecological malignancies
Update in
-
Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in women with gynaecological malignancies.Cochrane Database Syst Rev. 2017 Jun 29;6(6):CD007387. doi: 10.1002/14651858.CD007387.pub4. Cochrane Database Syst Rev. 2017. PMID: 28660687 Free PMC article. Review.
Abstract
Background: This is an updated version of the original Cochrane review published in Issue 1, 2010. Pelvic lymphadenectomy is associated with significant complications including lymphocyst formation and related morbidities. Retroperitoneal drainage using suction drains has been recommended as a method to prevent such complications. However, this policy has been challenged by the findings from recent studies.
Objectives: To assess the effects of retroperitoneal drainage versus no drainage after pelvic lymphadenectomy on lymphocyst formation and related morbidities in gynaecological cancer patients.
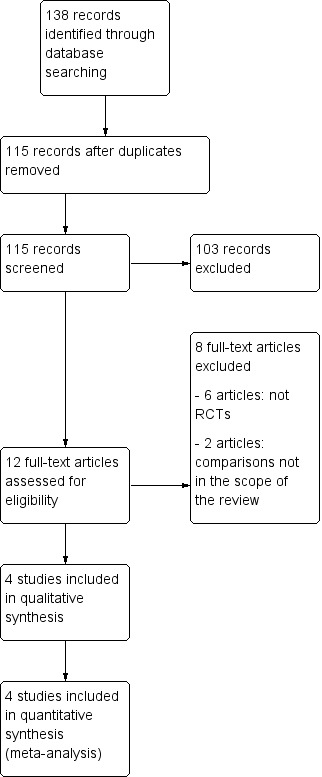
Search methods: We searched the Cochrane Gynaecological Cancer Specialised Register, the Cochrane Central Register of Controlled Trials (CENTRAL 2013, Issue 12) in The Cochrane Library, electronic databases MEDLINE (Nov Week 3, 2013), EMBASE (2014, week 1), and the citation lists of relevant publications. The latest searches were performed on 10 January 2014.
Selection criteria: Randomised controlled trials (RCTs) that compared the effect of retroperitoneal drainage versus no drainage after pelvic lymphadenectomy in gynaecological cancer patients. Retroperitoneal drainage was defined as placement of passive or active suction drains in pelvic retroperitoneal spaces. No drainage was defined as no placement of passive or active suction drains in pelvic retroperitoneal spaces.
Data collection and analysis: We assessed studies using methodological quality criteria. For dichotomous data, we calculated risk ratios (RRs) and 95% confidence intervals (CIs). We examined continuous data using mean difference (MD) and 95% CI.
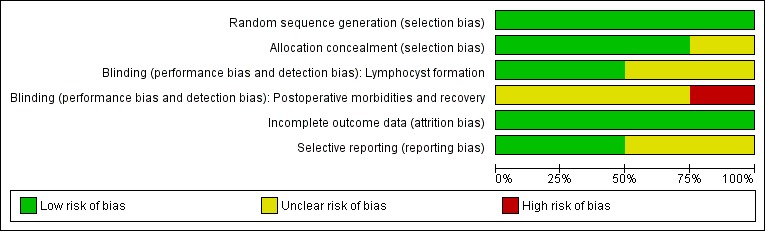
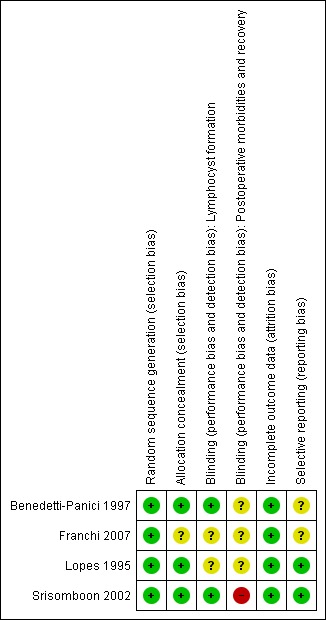
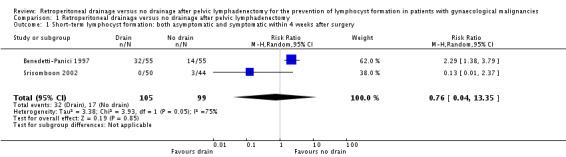
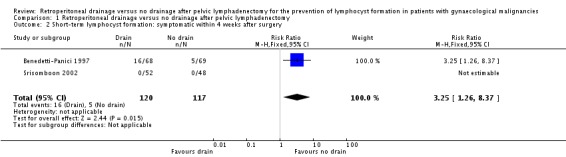
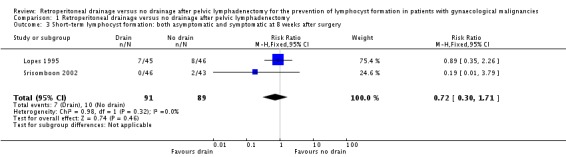
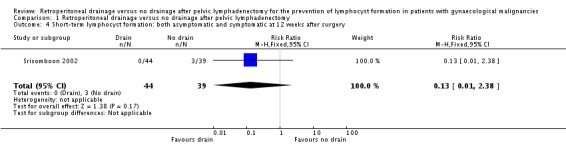
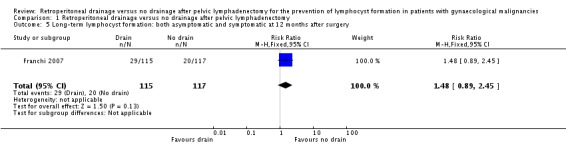
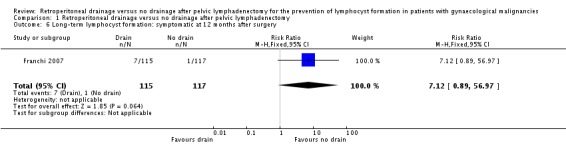
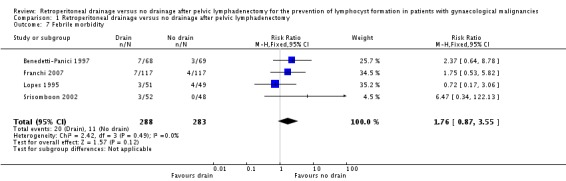
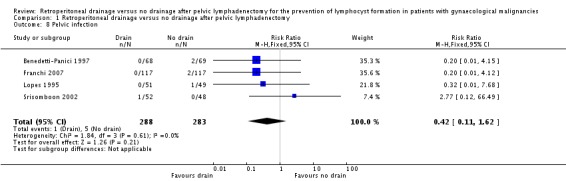
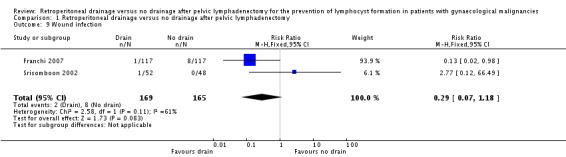
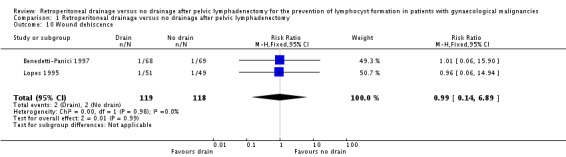
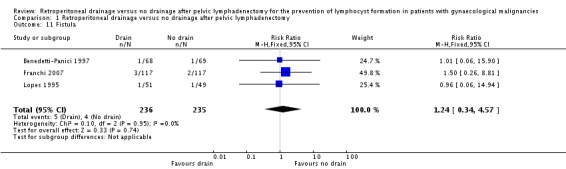
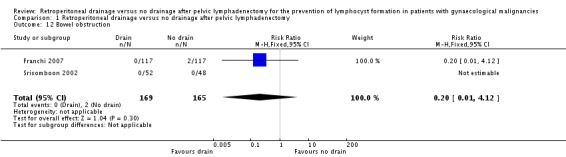
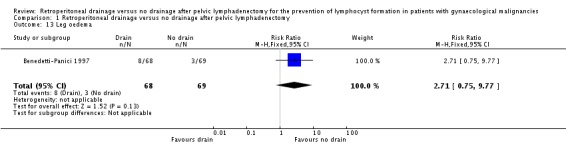
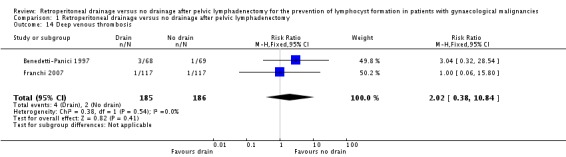
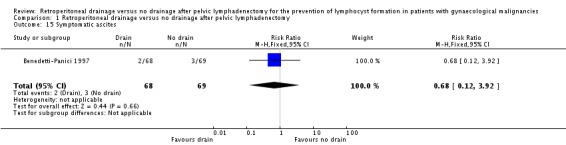
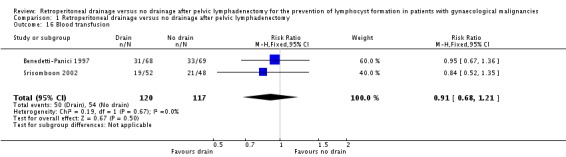
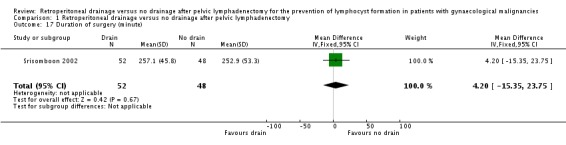
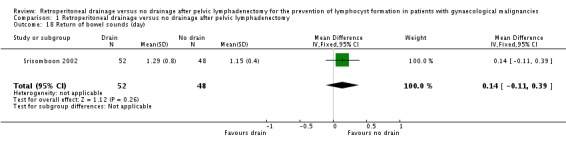
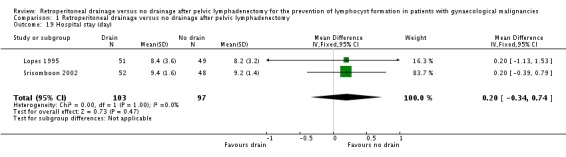
Main results: Since the last version of this review, no new studies have been identified for inclusion. The review included four studies with 571 participants. Considering the short-term outcomes (within four weeks after surgery), retroperitoneal drainage was associated with a comparable rate of overall lymphocyst formation when all methods of pelvic peritoneum management were considered together (two studies, 204 patients; RR 0.76, 95% CI 0.04 to 13.35). When the pelvic peritoneum was left open, the rates of overall lymphocyst formation (one study, 110 patients; RR 2.29, 95% CI 1.38 to 3.79) and symptomatic lymphocyst formation (one study, 137 patients; RR 3.25, 95% CI 1.26 to 8.37) were higher in the drained group. At 12 months after surgery, the rates of overall lymphocyst formation were comparable between the groups (one study, 232 patients; RR 1.48, 95% CI 0.89 to 2.45). However, there was a trend toward increased risk of symptomatic lymphocyst formation in the group with drains (one study, 232 patients; RR 7.12, 95% CI 0.89 to 56.97). The included trials were of low to moderate risk of bias.
Authors' conclusions: Placement of retroperitoneal tube drains has no benefit in prevention of lymphocyst formation after pelvic lymphadenectomy in patients with gynaecological malignancies. When the pelvic peritoneum is left open, the tube drain placement is associated with a higher risk of short and long-term symptomatic lymphocyst formation.
Conflict of interest statement
Kittipat Charoenkwan is a co‐author of the article 'A prospective randomized study comparing retroperitoneal drainage with no drainage and no peritonization following radical hysterectomy and pelvic lymphadenectomy for invasive cervical cancer' published in the
Figures
Update of
-
Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in patients with gynaecological malignancies.Cochrane Database Syst Rev. 2010 Jan 20;(1):CD007387. doi: 10.1002/14651858.CD007387.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2014 Jun 04;(6):CD007387. doi: 10.1002/14651858.CD007387.pub3. PMID: 20091631 Updated.
References
References to studies included in this review
-
- Benedetti‐Panici P, Maneschi F, Butillo G, D'Andrea G, Palumbo VS, Conte M, et al. A randomized study comparing retroperitoneal drainage with no drainage after lymphadenectomy in gynecologic malignancies. Gynecologic Oncology 1997;65:478‐82. - PubMed
-
- Franchi M, Trimbos J, Zanaboni F, Velden J, Reed N, Coens C, et al. Randomised trial of drains versus no drains following radical hysterectomy and pelvic lymph node dissection: a European Organisation for Research and Treatment of Cancer‐Gynaecological Cancer Group (EORTC‐GCG) study in 234 patients. European Journal of Cancer 2007;43:1265‐8. - PubMed
-
- Lopes AB, Hall JR, Monaghan JM. Drainage following radical hysterectomy and pelvic lymphadenectomy: dogma or need?. Obstetrics and Gynecology 1995;86:960‐3. - PubMed
-
- Srisomboon J, Phongnarisorn C, Suprasert P, Cheewakriangkrai C, Siriaree S, Charoenkwan K. A prospective randomized study comparing retroperitoneal drainage with no drainage and no peritonization following radical hysterectomy and pelvic lymphadenectomy for invasive cervical cancer. Journal of Obstetrics and Gynaecology Research 2002;28(3):149‐53. - PubMed
References to studies excluded from this review
-
- Bafna UD, Umadevi K, Savitha M. Closed suction drainage versus no drainage following pelvic lymphadenectomy for gynecological malignancies. International Journal of Gynecological Cancer 2001;11:143‐6. - PubMed
-
- Franchi M, Ghezzi F, Zanaboni F, Scarabelli C, Beretta P, Donadello N. Nonclosure of peritoneum at radical abdominal hysterectomy and pelvic node dissection: a randomized study. Obstetrics and Gynecology 1997;90(4):622‐7. - PubMed
-
- Jensen JK, Lucci JA 3rd, DiSaia PJ, Manetta A, Berman ML. To drain or not to drain: a retrospective study of closed‐suction drainage following radical hysterectomy with pelvic lymphadenectomy. Gynecologic Oncology 1993;51(1):46‐9. - PubMed
-
- Morice P, Lassau N, Pautier P, Haie‐Meder C, Lhomme C, Castaigne D. Retroperitoneal drainage after complete paraaortic lymphadenectomy for gynecologic cancer: a randomized trial. Obstetrics and Gynecology 2001;97(2):243‐7. - PubMed
-
- Orr JW Jr, Barter JF, Kilgore LC, Soong SJ, Shingleton HM, Hatch KD. Closed suction pelvic drainage after radical pelvic surgical procedures. American Journal of Obstetrics and Gynecology 1986;155(4):867‐71. - PubMed
Additional references
-
- Conte M, Benedetti‐Panici P, Guariglia L, Scambia G, Greggi S, Mancuso S. Pelvic lymphocele following radical para‐aortic and pelvic lymphadenectomy for cervical carcinoma: incidence rate and percutaneous management. Obstetrics and Gynecology 1990;76:268‐71. - PubMed
-
- Deeks JJ, Higgins JPT, Altman DG. Chapter 9: Analysing data and undertaking meta‐analyses. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.0 [updated September 2008]. Higgins JPT, Green S (editors). The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [Updated September 2008]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
-
- Ilancheran A, Monaghan J. Pelvic lymphocyst ‐ a 10‐year experience. Gynecologic Oncology 1988;29:333‐6. - PubMed
-
- Livingston W, Confer D, Smith R. Large lymphoceles resulting from retroperitoneal lymphadenectomy. Journal of Urology 1980;124:543‐6. - PubMed
References to other published versions of this review
-
- Charoenkwan K, Kietpeerakool C. Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in patients with gynaecological malignancies. Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD007387.pub2] - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources