

Protein changes contributing to right ventricular cardiomyocyte diastolic dysfunction in pulmonary arterial hypertension
- PMID: 24895160
- PMCID: PMC4309054
- DOI: 10.1161/JAHA.113.000716
Protein changes contributing to right ventricular cardiomyocyte diastolic dysfunction in pulmonary arterial hypertension
Abstract
Background: Right ventricular (RV) diastolic function is impaired in patients with pulmonary arterial hypertension (PAH). Our previous study showed that elevated cardiomyocyte stiffness and myofilament Ca(2+) sensitivity underlie diastolic dysfunction in PAH. This study investigates protein modifications contributing to cellular diastolic dysfunction in PAH.
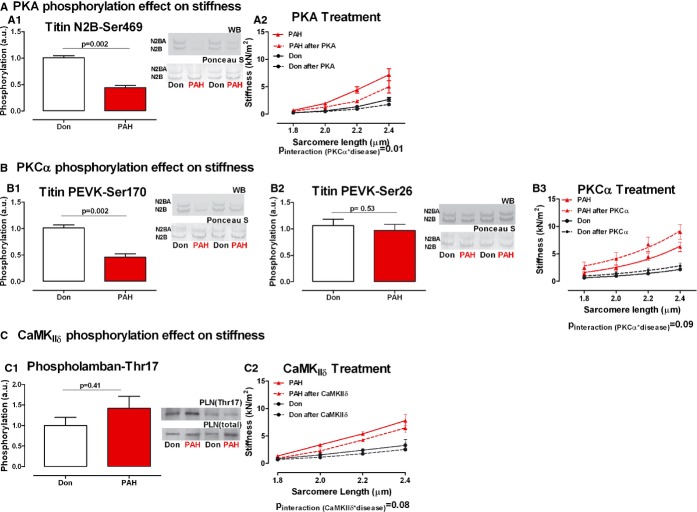
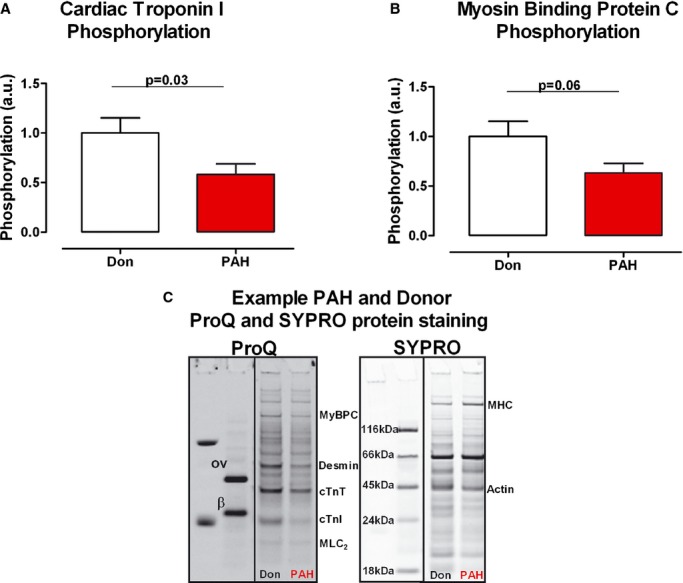
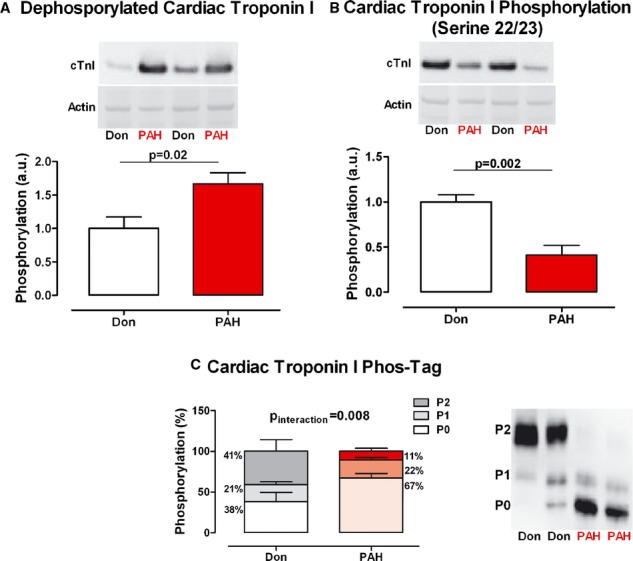
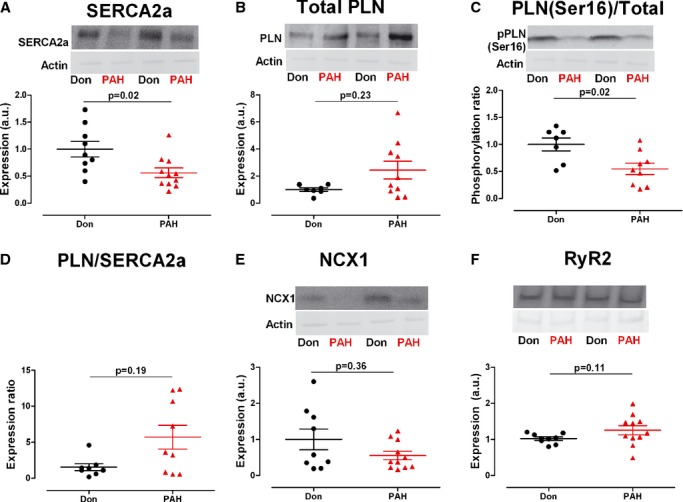
Methods and results: RV samples from PAH patients undergoing heart-lung transplantation were compared to non-failing donors (Don). Titin stiffness contribution to RV diastolic dysfunction was determined by Western-blot analyses using antibodies to protein-kinase-A (PKA), Cα (PKCα) and Ca(2+)/calmoduling-dependent-kinase (CamKIIδ) titin and phospholamban (PLN) phosphorylation sites: N2B (Ser469), PEVK (Ser170 and Ser26), and PLN (Thr17), respectively. PKA and PKCα sites were significantly less phosphorylated in PAH compared with donors (P<0.0001). To test the functional relevance of PKA-, PKCα-, and CamKIIδ-mediated titin phosphorylation, we measured the stiffness of single RV cardiomyocytes before and after kinase incubation. PKA significantly decreased PAH RV cardiomyocyte diastolic stiffness, PKCα further increased stiffness while CamKIIδ had no major effect. CamKIIδ activation was determined indirectly by measuring PLN Thr17phosphorylation level. No significant changes were found between the groups. Myofilament Ca(2+) sensitivity is mediated by sarcomeric troponin I (cTnI) phosphorylation. We observed increased unphosphorylated cTnI in PAH compared with donors (P<0.05) and reduced PKA-mediated cTnI phosphorylation (Ser22/23) (P<0.001). Finally, alterations in Ca(2+)-handling proteins contribute to RV diastolic dysfunction due to insufficient diastolic Ca(2+) clearance. PAH SERCA2a levels and PLN phosphorylation were significantly reduced compared with donors (P<0.05).
Conclusions: Increased titin stiffness, reduced cTnI phosphorylation, and altered levels of phosphorylation of Ca(2+) handling proteins contribute to RV diastolic dysfunction in PAH.
Keywords: diastole; pulmonary heart disease.
© 2014 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Rain S, Handoko ML, Trip P, Gan CT‐J, Westerhof N, Stienen GJ, Paulus WJ, Ottenheijm CAC, Marcus JT, Dorfmüller P, Guignabert C, Humbert M, Macdonald P, Dos Remedios C, Postmus PE, Saripalli C, Hidalgo CG, Granzier HL, Vonk‐Noordegraaf A, van der Velden J, de Man FS. Right ventricular diastolic impairment in patients with pulmonary arterial hypertension. Circulation. 2013; 128:2016-2025. - PubMed
-
- De Tombe PP, Granzier HL. The cytoskeleton and the cellular transduction of mechanical strain in the heart: a special issue. Pflugers Arch. 2011; 462:1-2. - PubMed
-
- Fukuda N, Granzier HL, Ishiwata S, Kurihara S. Physiological functions of the giant elastic protein titin in mammalian striated muscle. J Physiol Sci. 2008; 58:151-159. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
