

CT and MRI of primary and metastatic fibrolamellar carcinoma: a case series of 37 patients
- PMID: 24896196
- PMCID: PMC4112400
- DOI: 10.1259/bjr.20140024
CT and MRI of primary and metastatic fibrolamellar carcinoma: a case series of 37 patients
Abstract
Objective: Fibrolamellar carcinoma (FLC) is a rare disease, with limited radiographic reported information. We assessed the imaging patterns of primary and metastatic FLC.
Methods: CT and MR examinations of patients with FLC were retrospectively reviewed. Imaging features were assessed for primary and recurrent liver tumours, including dimension, enhancement characteristics, and presence or absence of central scars. Locations of nodal and extranodal metastases were also recorded.
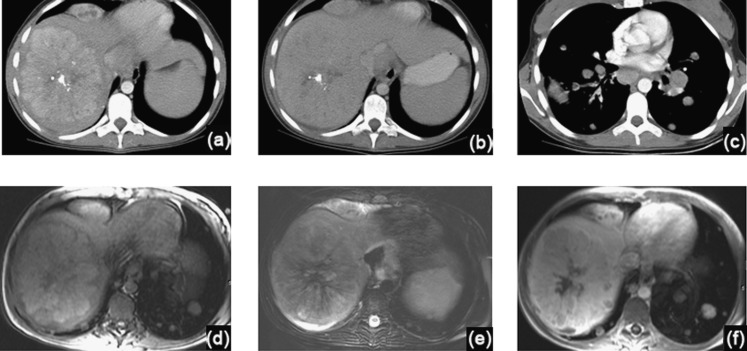
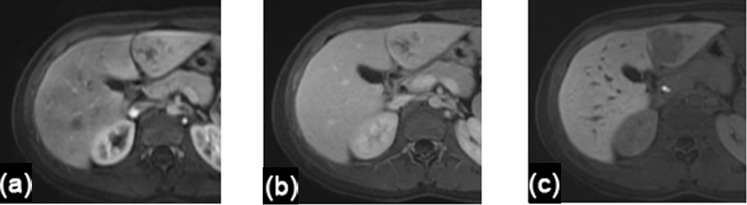
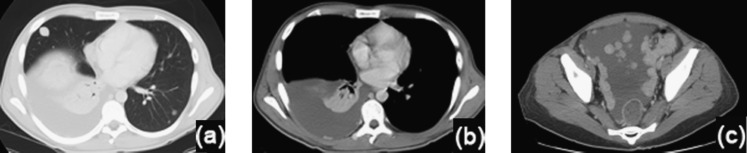
Results: Of 37 patients (18 males and 19 females; average age, 23.5 years) with FLC, 24 had imaging of their primary tumour; 13 had metastases at presentation and 7 developed metastases on follow-up. The remaining 13 patients had follow-up imaging of metastatic disease. Primary FLC had a mean diameter >11 cm, with central scars in ten (46%) patients. Most tumours enhanced heterogeneously (96%) and showed arterial enhancement (81%). On MRI, 62% of FLCs were hypointense on T1 weighted imaging and 54% were hyperintense on T2 weighted imaging. 13 patients (54%) had nodal metastases at presentation, mostly in the upper abdomen (92%) and commonly in the chest (38%). Extrahepatic metastases were most frequently pulmonary or peritoneal. Predominantly small and homogeneous intrahepatic recurrences were detected on follow-up in 15 patients.
Conclusion: FLC often presents as a large hepatic tumour with nodal and distant metastases. Thoracic adenopathy and lung metastases were frequently found in our series, suggesting the need for pre-operative and follow-up chest imaging.
Advances in knowledge: Thoracic nodal and lung metastases are common in FLC; therefore, dedicated chest imaging should be part of the evaluation of a patient with FLC.
Figures




Similar articles
-
Imaging features of fibrolamellar hepatocellular carcinoma in gadoxetic acid-enhanced MRI.Cancer Imaging. 2018 Mar 1;18(1):9. doi: 10.1186/s40644-018-0143-y. Cancer Imaging. 2018. PMID: 29490696 Free PMC article.
-
[Surgical therapy of hepatic fibrolamellar carcinoma].Ann Ital Chir. 2007 Jan-Feb;78(1):53-8. Ann Ital Chir. 2007. PMID: 17518332 Italian.
-
Imaging features of primary and metastatic alveolar soft part sarcoma: single institute experience in 25 patients.Br J Radiol. 2014 Apr;87(1036):20130719. doi: 10.1259/bjr.20130719. Epub 2014 Feb 17. Br J Radiol. 2014. PMID: 24641199 Free PMC article.
-
State-of-the-art MR Imaging of Uncommon Hepatocellular Tumours: Fibrolamellar Hepatocellular Carcinoma and Combined Hepatocellularcholangiocarcinoma.Curr Med Imaging Rev. 2019;15(3):269-280. doi: 10.2174/1573405614666180927113622. Curr Med Imaging Rev. 2019. PMID: 31989878 Review.
-
Extrahepatic metastases of hepatocellular carcinoma: A spectrum of imaging findings.Can Assoc Radiol J. 2014 Feb;65(1):60-6. doi: 10.1016/j.carj.2013.05.004. Epub 2013 Nov 13. Can Assoc Radiol J. 2014. PMID: 24239313 Review.
Cited by
-
Intracranial metastasis in fibrolamellar hepatocellular carcinoma.Pediatr Blood Cancer. 2018 Apr;65(4):10.1002/pbc.26919. doi: 10.1002/pbc.26919. Epub 2017 Dec 29. Pediatr Blood Cancer. 2018. PMID: 29286561 Free PMC article.
-
Fibrolamellar Hepatocellular Carcinoma (FLHCC) in a Young Patient Presenting With Nausea and Vomiting After a Greasy Meal.Cureus. 2024 Mar 9;16(3):e55863. doi: 10.7759/cureus.55863. eCollection 2024 Mar. Cureus. 2024. PMID: 38595871 Free PMC article.
-
Genome and transcriptome profiling of fibrolamellar hepatocellular carcinoma demonstrates p53 and IGF2BP1 dysregulation.PLoS One. 2017 May 9;12(5):e0176562. doi: 10.1371/journal.pone.0176562. eCollection 2017. PLoS One. 2017. PMID: 28486549 Free PMC article.
-
Imaging features of fibrolamellar hepatocellular carcinoma in gadoxetic acid-enhanced MRI.Cancer Imaging. 2018 Mar 1;18(1):9. doi: 10.1186/s40644-018-0143-y. Cancer Imaging. 2018. PMID: 29490696 Free PMC article.
-
Contemporary management of fibrolamellar hepatocellular carcinoma: diagnosis, treatment, outcome, prognostic factors, and recent developments.World J Surg Oncol. 2016 May 23;14(1):151. doi: 10.1186/s12957-016-0903-8. World J Surg Oncol. 2016. PMID: 27215576 Free PMC article. Review.
References
-
- Kakar S, Burgart LJ, Batts KP, Garcia J, Jain D, Ferrell LD. Clinicopathologic features and survival in fibrolamellar carcinoma: comparison with conventional hepatocellular carcinoma with and without cirrhosis. Mod Pathol 2005; 18: 1417–23. - PubMed
-
- Hemming AW, Langer B, Sheiner P, Greig PD, Taylor BR. Aggressive surgical management of fibrolamellar hepatocellular carcinoma. J Gastrointest Surg 1997; 1: 342–6. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
