

Is there a paradox in obesity?
- PMID: 24896249
- PMCID: PMC4048872
- DOI: 10.1097/CRD.0000000000000004
Is there a paradox in obesity?
Abstract
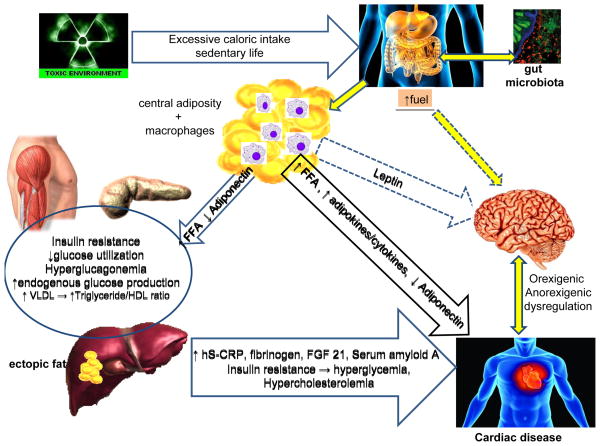
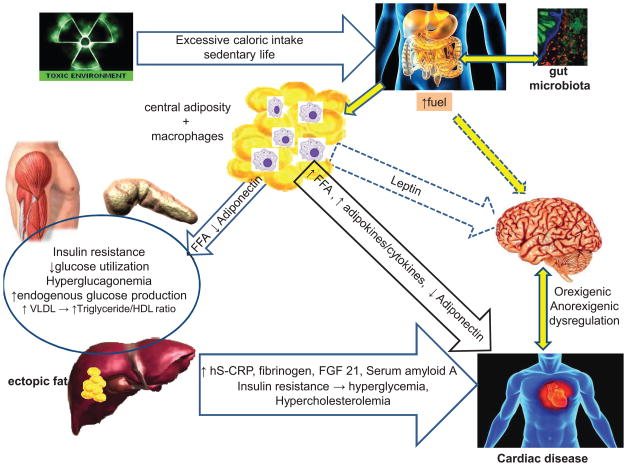
In an industrialized society, the increase in obesity incidence has led to an increase in premature morbidity and mortality rates. There is a relationship between body mass index (BMI) and the increased incidence of hypertension, dyslipidemia, type 2 diabetes mellitus, and cardiovascular disease, an increase in mortality. However, obese individuals with these conditions may have better outcomes than their lean counterparts, thus the term "obesity paradox." Most studies supporting this paradox are cross-sectional and do not take into account the quantity or type of adiposity, the disease severity, and comorbidities. Although BMI is an indicator of the amount of body fat, it does not differentiate between adiposity types. Adipocytes that are highly functional have good fuel storage capacity are different from adipocytes found in visceral obesity, which are poorly functioning, laden with macrophages, and causing low-grade inflammation. Individuals with high BMI may be physically fit and have a lower mortality risk when compared with individuals with a lower BMI and poorly functioning adiposity. We review the complexity of adipose tissue and its location, function, metabolic implications, and role in cardiovascular morbidity and mortality. The terminology "obesity paradox" may reflect a lack of understanding of the complex pathophysiology of obesity and the association between adiposity and cardiovascular disease.
Conflict of interest statement
Figures
References
-
- Gruberg L, Weissman NJ, Waksman R, et al. The impact of obesity on the short-term and long-term outcomes after percutaneous coronary intervention: The obesity paradox? J Am Coll Cardiol. 2002;39:578–584. - PubMed
-
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999–2008. JAMA. 2010;303:235–241. - PubMed
-
- O’Rahilly S. Human genetics illuminates the paths to metabolic disease. Nature. 2009;462:307–314. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
