

Allopurinol therapy in gout patients does not associate with beneficial cardiovascular outcomes: a population-based matched-cohort study
- PMID: 24897240
- PMCID: PMC4045898
- DOI: 10.1371/journal.pone.0099102
Allopurinol therapy in gout patients does not associate with beneficial cardiovascular outcomes: a population-based matched-cohort study
Abstract
Introduction: Previous studies have shown an association between gout and/or hyperuricemia and a subsequent increase in cardiovascular disease (CVD) outcomes. Allopurinol reduces vascular oxidative stress, ameliorates inflammatory state, improves endothelial function, and prevents atherosclerosis progression. Accordingly, we tested the hypothesis that a positive association between allopurinol therapy in gout patients and future cardiovascular outcomes is present using a population-based matched-cohort study design.
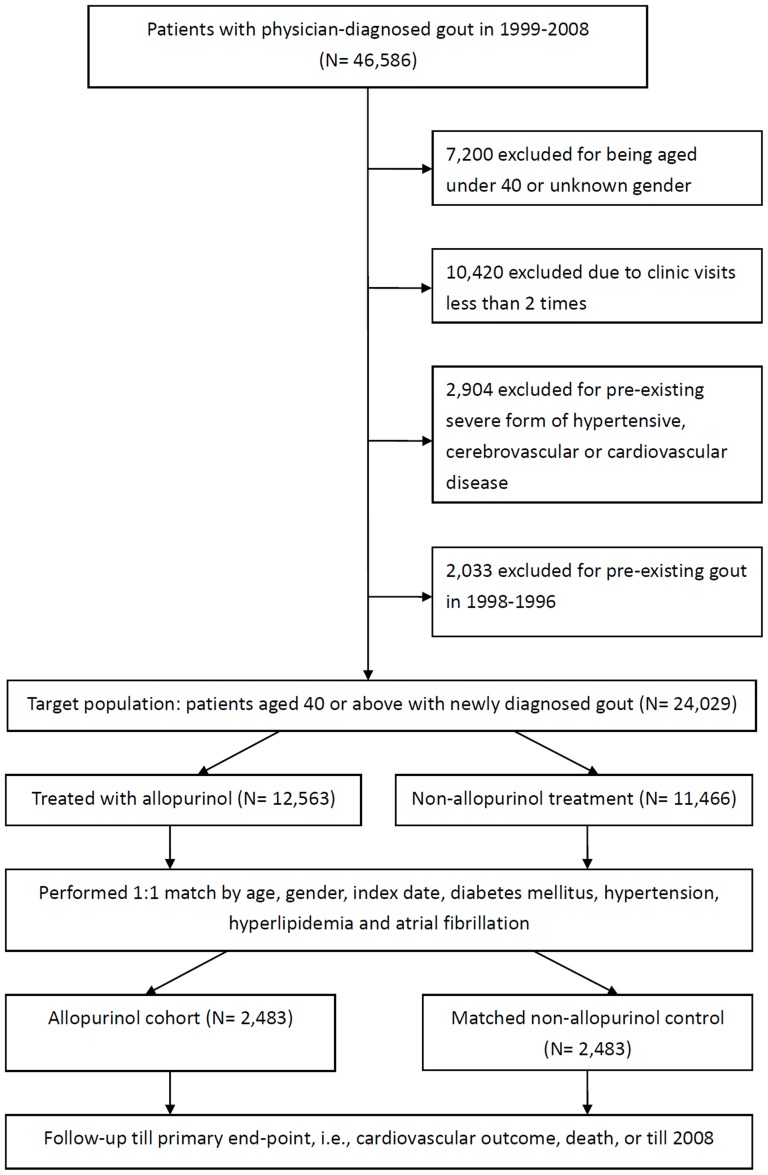
Methods: Patients aged ≥40 years with newly diagnosed gout having no pre-existing severe form of CVD were separated into allopurinol (n = 2483) and non-allopurinol (n = 2483) groups after matching for age, gender, index date, diabetes mellitus, hypertension, hyperlipidemia, and atrial fibrillation. The two groups were also balanced in terms of uric acid nephrolithiasis, acute kidney injury, hepatitis, and Charlson comorbidity index.
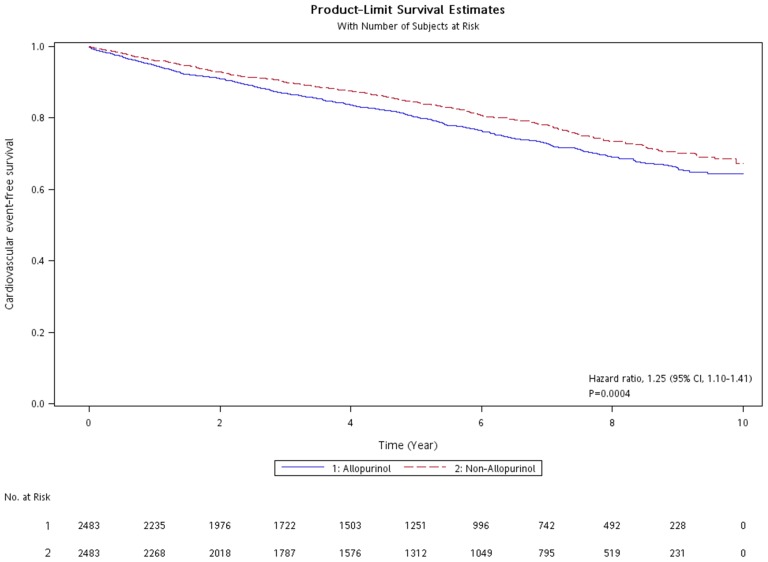
Results: With a median follow-up time of 5.25 years, the allopurinol group had a modest increase in cardiovascular risk [relative risk, 1.20; 95% confidence interval (CI), 1.08-1.34]. A Cox proportional hazard model adjusted for chronic kidney disease, uremia, and gastric ulcer gave a hazard ratio (HR) for cardiovascular outcomes of 1.25 (95% CI, 1.10-1.41) in gout patients receiving allopurinol compared with the non-allopurinol group. In further analysis of patients receiving urate-lowering therapy, the uricosuric agent group (n = 1713) had an adjusted HR of 0.83 (0.73-0.95) for cardiovascular events compared with the allopurinol group.
Conclusions: The current population-based matched-cohort study did not support the association between allopurinol therapy in gout patients with normal risk for cardiovascular sequels and beneficial future cardiovascular outcomes. Several important risk factors for cardiovascular disease, such as smoking, alcohol consumption, body mass index, blood pressure were not obtainable in the current retrospective cohort study, thus could potentially bias the effect estimate.
Conflict of interest statement
Figures
References
-
- Bhansing KJ, van Bon L, Janssen M, Radstake TR (2010) Gout: a clinical syndrome illustrated and discussed. Neth J Med 68: 352–359. - PubMed
-
- Zhu Y, Pandya BJ, Choi HK (2011) Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007-2008. Arthritis Rheum 63: 3136–3141. - PubMed
-
- Kanbay M, Sanchez-Lozada LG, Franco M, Madero M, Solak Y, et al. (2011) Microvascular disease and its role in the brain and cardiovascular system: a potential role for uric acid as a cardiorenal toxin. Nephrol Dial Transplant 26: 430–437. - PubMed
-
- Puddu P, Puddu GM, Cravero E, Vizioli L, Muscari A (2012) Relationships among hyperuricemia, endothelial dysfunction and cardiovascular disease: molecular mechanisms and clinical implications. J Cardiol 59: 235–242. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
