

Risk factors for recurrence, complications and mortality in Clostridium difficile infection: a systematic review
- PMID: 24897375
- PMCID: PMC4045753
- DOI: 10.1371/journal.pone.0098400
Risk factors for recurrence, complications and mortality in Clostridium difficile infection: a systematic review
Erratum in
- PLoS One. 2014;9(8):e107420
Abstract
Background: Clostridium difficile infection (CDI) can lead to complications, recurrence, and death. Numerous studies have assessed risk factors for these unfavourable outcomes, but systematic reviews or meta-analyses published so far were limited in scope or in quality.
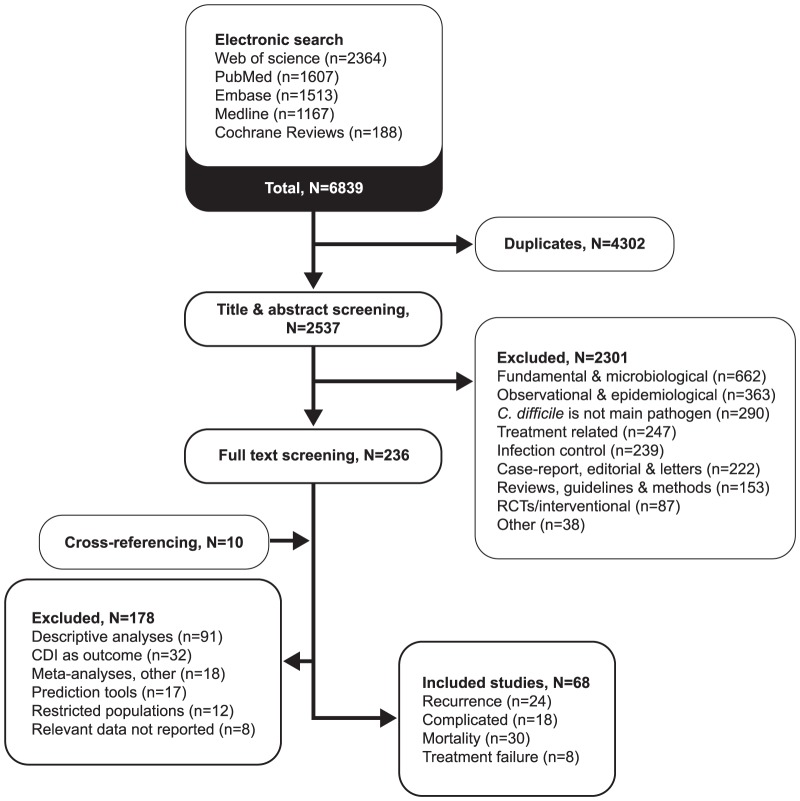
Methods: A systematic review was completed according to PRISMA guidelines. An electronic search in five databases was performed. Studies published until October 2013 were included if risk factors for at least one CDI outcome were assessed with multivariate analyses.
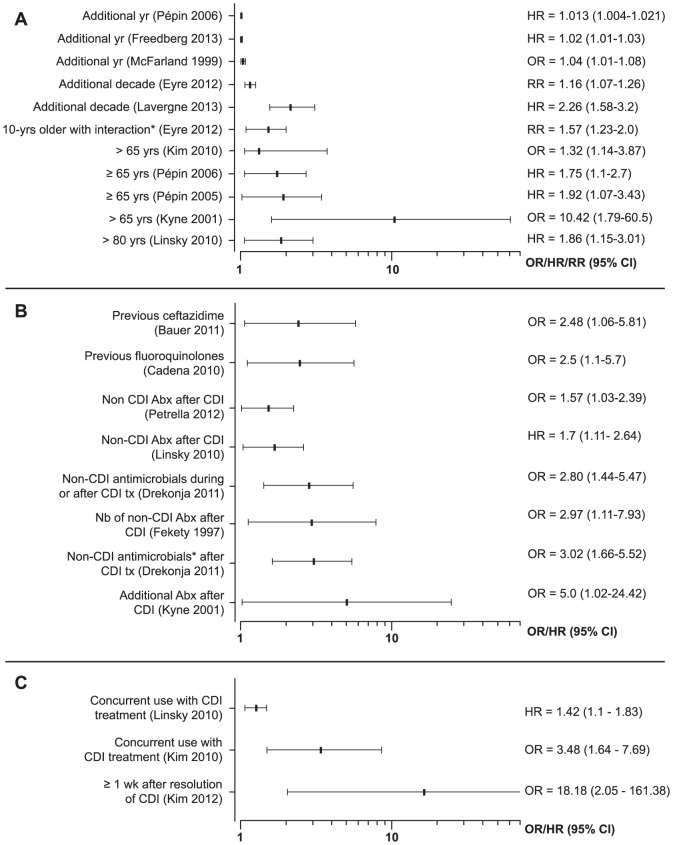
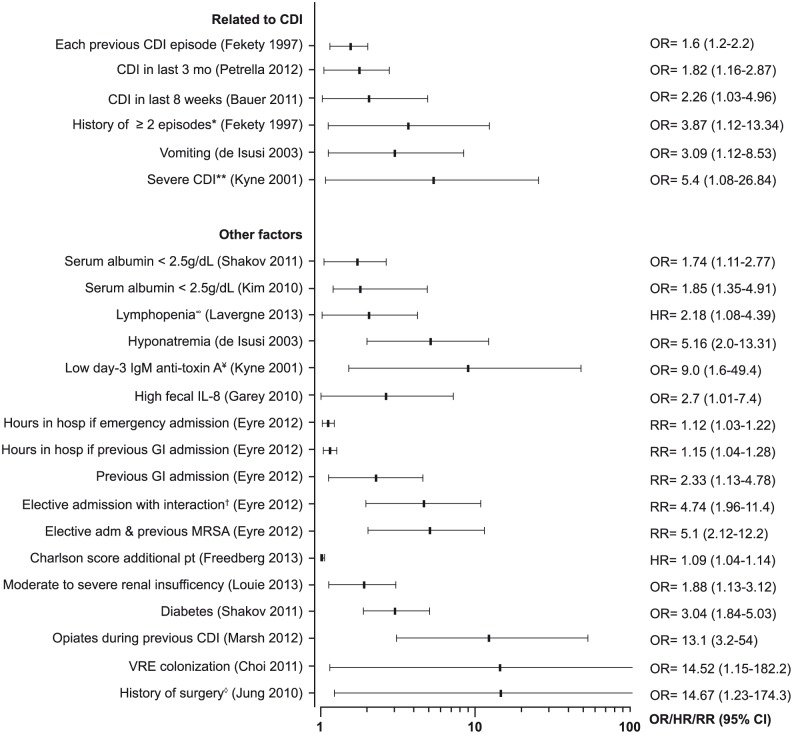
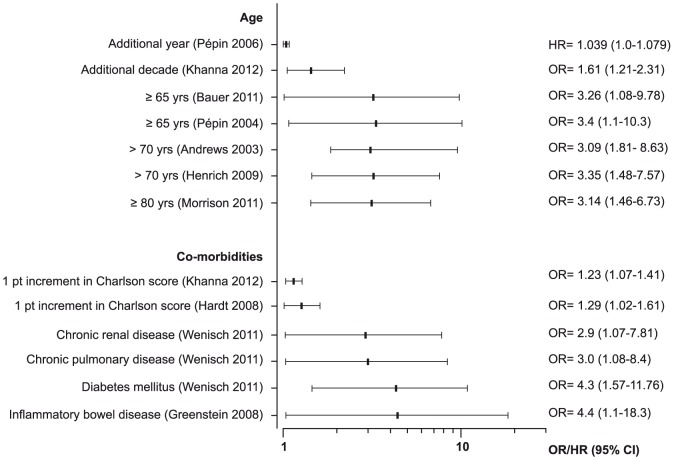
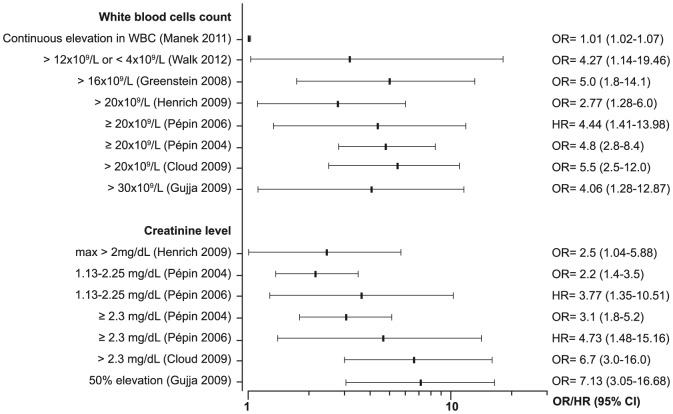
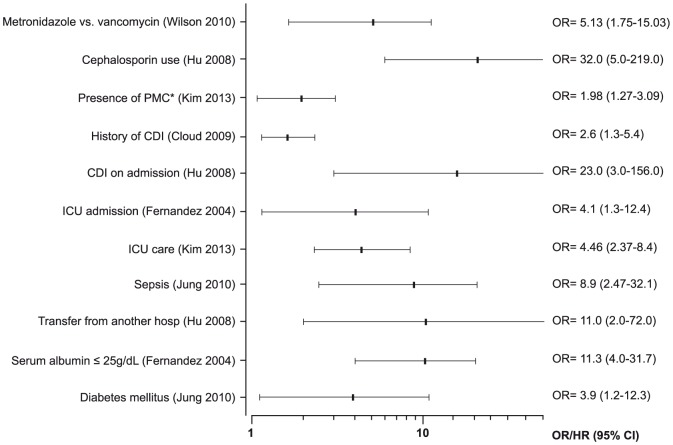
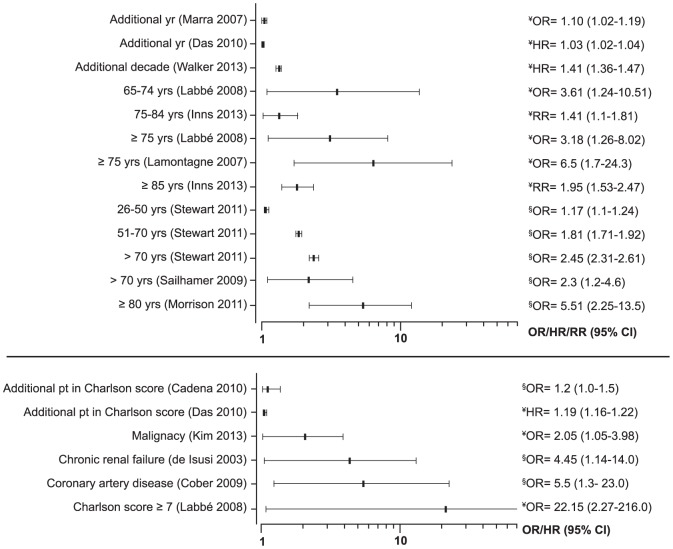
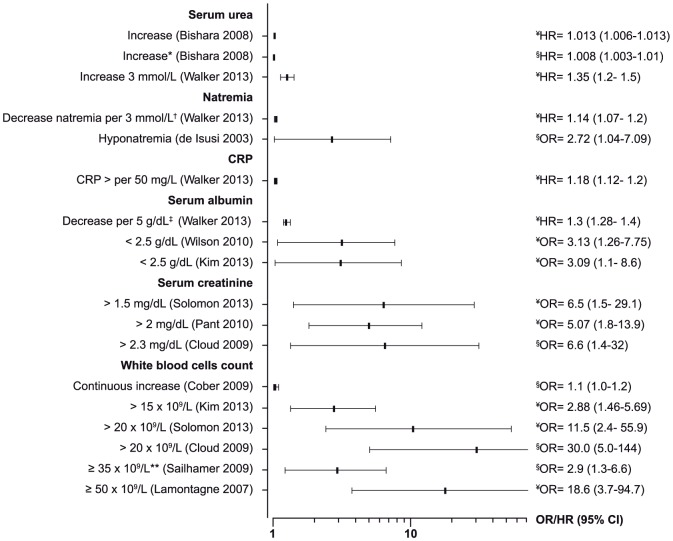
Results: 68 studies were included: 24 assessed risk factors for recurrence, 18 for complicated CDI, 8 for treatment failure, and 30 for mortality. Most studies accounted for mortality in the definition of complicated CDI. Important variables were inconsistently reported, such as previous episodes and use of antibiotics. Substantial heterogeneity and methodological limitations were noted, mainly in the sample size, the definition of the outcomes and periods of follow-up, precluding a meta-analysis. Older age, use of antibiotics after diagnosis, use of proton pump inhibitors, and strain type were the most frequent risk factors for recurrence. Older age, leucocytosis, renal failure and co-morbidities were frequent risk factors for complicated CDI. When considered alone, mortality was associated with age, co-morbidities, hypo-albuminemia, leucocytosis, acute renal failure, and infection with ribotype 027.
Conclusion: Laboratory parameters currently used in European and American guidelines to define patients at risk of a complicated CDI are adequate. Strategies for the management of CDI should be tailored according to the age of the patient, biological markers of severity, and underlying co-morbidities.
Conflict of interest statement
Figures
References
-
- McDonald LC, Coignard B, Dubberke E, Song X, Horan T, et al. (2007) Recommendations for surveillance of Clostridium difficile-associated disease. Infect Control Hosp Epidemiol 28: 140–5. - PubMed
-
- Aslam S, Hamill RJ, Musher DM (2005) Treatment of Clostridium difficile-associated disease: old therapies and new strategies. Lancet Infect Dis 5: 549–57. - PubMed
-
- Rupnik M, Wilcox MH, Gerding DN (2009) Clostridium difficile infection: new developments in epidemiology and pathogenesis. Nat Rev Microbiol 7: 526–36. - PubMed
-
- Nelson RL, Kelsey P, Leeman H, Meardon N, Patel H, et al. (2011) Antibiotic treatment for Clostridium difficile-associated diarrhea in adults. Cochrane Database Syst Rev 9: CD004610. - PubMed
-
- Hensgens MP, Goorhuis A, Dekkers OM, Kuijper EJ (2012) Time interval of increased risk for Clostridium difficile infection after exposure to antibiotics. J Antimicrob Chemother 67: 742–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
