

Risk of stroke in patients with rheumatism: a nationwide longitudinal population-based study
- PMID: 24898360
- PMCID: PMC4046260
- DOI: 10.1038/srep05110
Risk of stroke in patients with rheumatism: a nationwide longitudinal population-based study
Abstract
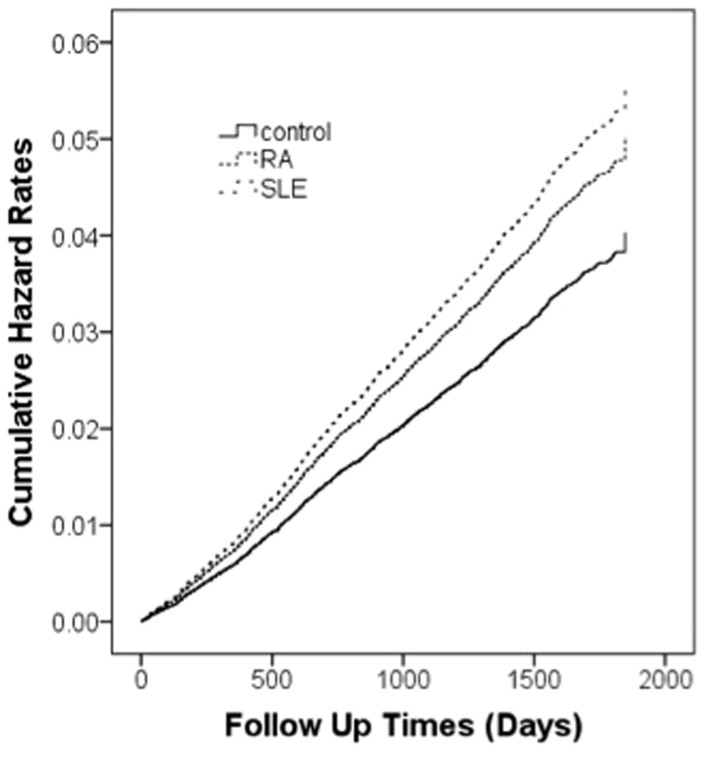
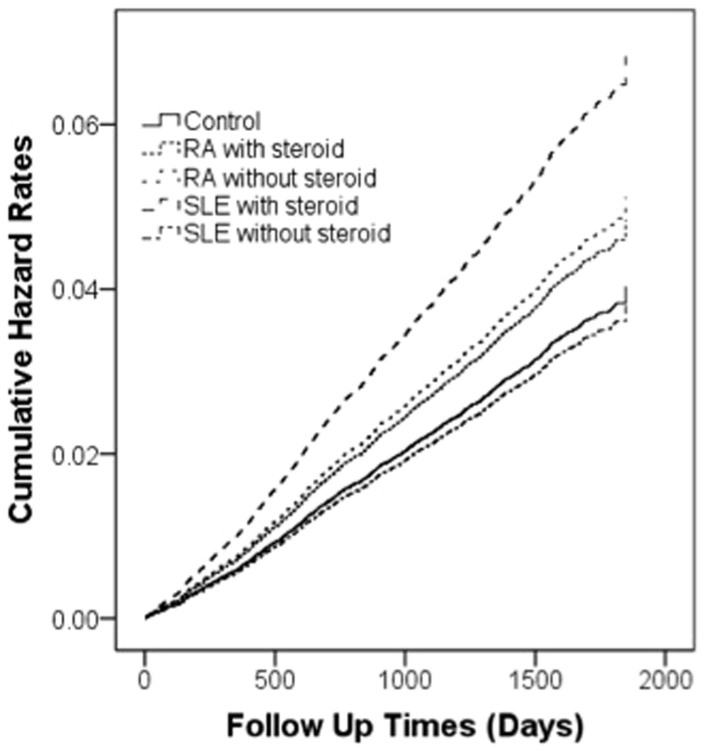
The aim of this study was to investigate rheumatoid arthritis (RA), and systemic lupus erythematous (SLE) as risk factors for stroke. The study was analyzed by Using the Taiwan Longitudinal Health Insurance Database 2005 (LHID2005), this cohort study investigated patients with a recorded diagnosis of RA (N = 6114), and SLE (N = 621) between January 1, 2004, and December 31, 2007, with age-matched controls (1:4) (for RA, N = 24456; SLE, N = 2484). We used Cox proportional-hazard regressions to evaluate the hazard ratios (HRs) after adjusting confounding factors. Our study found 383 of 6114 RA patients, experienced stroke during the 20267 person-year follow-up period. The adjusted HR of stroke for RA patients was 1.24 (95% CI, 1.11 to 1.39), and for SLE patients was 1.88 (95% CI, 1.08 to 3.27). When steroid was added as additional confounding factor, the adjusted HR of ischemic stroke for RA patients was 1.32 (95% CI, 1.15 to 1.50), and for SLE patients was 1.31 (95% CI, 0.51 to 3.34). In conclusion, the rheumatic diseases of RA, and SLE are all risk factors for stroke. After controlled the effect of steroid prescription, RA is risk factor for ischemic stroke.
Figures
References
-
- Ra G. S., Yoo J. C., Kang C. J. & Kim Y. S. Microfabricated in-channel structured polydimethylsiloxane microfluidic system for a lab-on-a-chip. J Nanosci Nanotechnol 8, 4588–4592 (2008). - PubMed
-
- Donnan G. A., Fisher M., Macleod M. & Davis S. M. Stroke. Lancet 371, 1612–1623, 10.1016/S0140-6736(08)60694-7 (2008). - PubMed
-
- Jakovljevic D. et al. Socioeconomic status and ischemic stroke: The FINMONICA Stroke Register. Stroke 32, 1492–1498 (2001). - PubMed
-
- Chen P. C., Tseng T. C., Hsieh J. Y. & Lin H. W. Association between stroke and patients with pelvic inflammatory disease: a nationwide population-based study in taiwan. Stroke 42, 2074–2076, STROKEAHA.110.612655 [pii] 10.1161/STROKEAHA.110.612655 (2011). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
