

Comorbidity profiles and inpatient outcomes during hospitalization for heart failure: an analysis of the U.S. Nationwide inpatient sample
- PMID: 24898986
- PMCID: PMC4057902
- DOI: 10.1186/1471-2261-14-73
Comorbidity profiles and inpatient outcomes during hospitalization for heart failure: an analysis of the U.S. Nationwide inpatient sample
Abstract
Background: Treatment of heart failure (HF) is particularly complex in the presence of comorbidities. We sought to identify and associate comorbidity profiles with inpatient outcomes during HF hospitalizations.
Methods: Latent mixture modeling was used to identify common profiles of comorbidities during adult hospitalizations for HF from the 2009 Nationwide Inpatient Sample (n = 192,327).
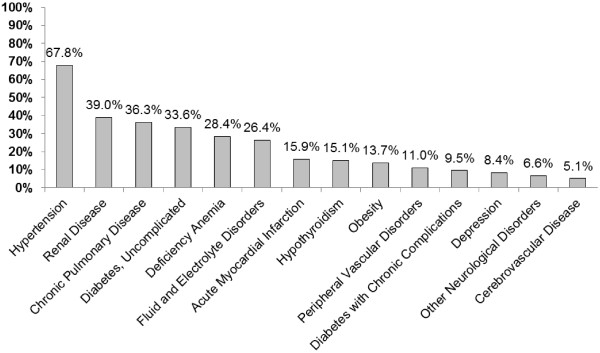
Results: Most discharges were characterized by "common" comorbidities. A "lifestyle" profile was characterized by a high prevalence of uncomplicated diabetes, hypertension, chronic pulmonary disorders and obesity. A "renal" profile had the highest prevalence of renal disease, complicated diabetes, and fluid and electrolyte imbalances. A "neurovascular" profile represented the highest prevalence of cerebrovascular disease, paralysis, myocardial infarction and peripheral vascular disease. Relative to the common profile, the lifestyle profile was associated with a 15% longer length of stay (LOS) and 12% greater cost, the renal profile was associated with a 30% higher risk of death, 27% longer LOS and 24% greater cost, and the neurovascular profile was associated with a 45% higher risk of death, 34% longer LOS and 37% greater cost (all p < 0.001).
Conclusions: Comorbidity profiles are helpful in identifying adults at higher risk of death, longer length of stay, and accumulating greater costs during hospitalizations for HF.
Figures

References
-
- Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA, Mancini DM, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):1977–2016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
