

2-methoxyestradiol plasma levels are associated with clinical severity indices and biomarkers of preeclampsia
- PMID: 24899468
- PMCID: PMC4287600
- DOI: 10.1177/1933719114537716
2-methoxyestradiol plasma levels are associated with clinical severity indices and biomarkers of preeclampsia
Abstract
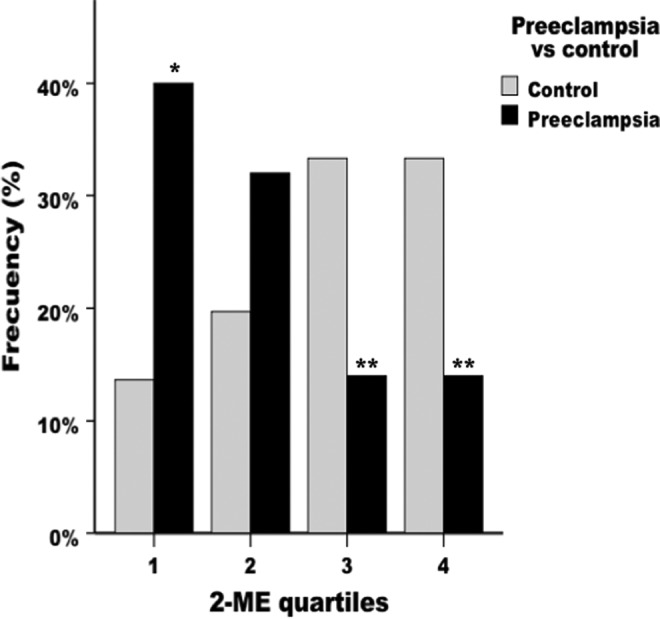
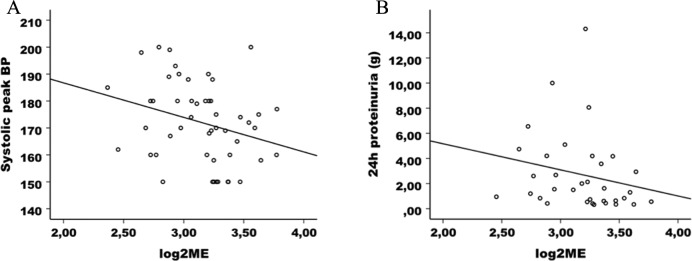
We investigated whether clinical severity indices and biomarkers for preeclampsia (PE) are associated with low plasmatic 2-methoxyestradiol (2ME) in the third trimester of gestation. Blood was collected from 53 women with PE and 73 control pregnant women before parturition. The concentration of 2ME was significantly higher in controls than in patients with PE (2906.43 ± 200.69 pg/mL vs 1818.41 ± 189.25 pg/mL). The risk of PE decreased as 2ME levels increased. The 2ME values were negatively correlated with systolic peak arterial pressure and proteinuria in PE. Additionally, those women with PE with lower 2ME had a more serious clinical situation and needed a more aggressive therapy. Finally, 2ME levels (in patients with PE and total population) were significantly correlated with concentrations of soluble fms-like tyrosine kinase 1 and placental growth factor . Summarizing, patients with PE had lower 2ME levels that were correlated with different clinical indices and biomarkers of severity, indicating that 2ME could be taken into account for the clinical management of this syndrome.
Keywords: PlGF; catechol-O-methyltransferase; estrogen; pregnancy; sFlt-1.
© The Author(s) 2014.
Conflict of interest statement
Figures



References
-
- Ghulmiyyah L, Sibai B. Maternal mortality from preeclampsia/eclampsia. Semin Perinatol. 2012;36 (1):56–59. - PubMed
-
- Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33 (3):130–137. - PubMed
-
- Shenoy V, Kanasaki K, Kalluri R. Pre-eclampsia: connecting angiogenic and metabolic pathways. Trends Endocrinol Metab. 2010;21(9):529–536. - PubMed
-
- Verlohren S, Stepan H, Dechend R. Angiogenic growth factors in the diagnosis and prediction of pre-eclampsia. Clin Sci (Lond). 2012;122 (2):43–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
