

Benefits and harms in clinical trials of duloxetine for treatment of major depressive disorder: comparison of clinical study reports, trial registries, and publications
- PMID: 24899650
- PMCID: PMC4045316
- DOI: 10.1136/bmj.g3510
Benefits and harms in clinical trials of duloxetine for treatment of major depressive disorder: comparison of clinical study reports, trial registries, and publications
Abstract
Objective: To determine, using research on duloxetine for major depressive disorder as an example, if there are inconsistencies between protocols, clinical study reports, and main publicly available sources (journal articles and trial registries), and within clinical study reports themselves, with respect to benefits and major harms.
Design: Data on primary efficacy analysis and major harms extracted from each data source and compared.
Setting: Nine randomised placebo controlled trials of duloxetine (total 2878 patients) submitted to the European Medicines Agency (EMA) for marketing approval for major depressive disorder.
Data sources: Clinical study reports, including protocols as appendices (total 13,729 pages), were obtained from the EMA in May 2011. Journal articles were identified through relevant literature databases and contacting the manufacturer, Eli Lilly. Clinicaltrials.gov and the manufacturer's online clinical trial registry were searched for trial results.
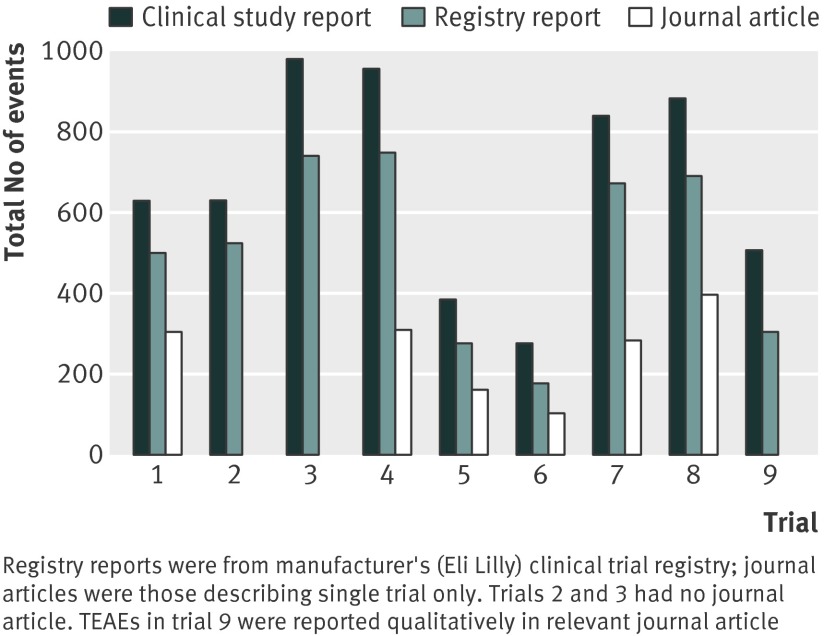
Results: Clinical study reports fully described the primary efficacy analysis and major harms (deaths (including suicides), suicide attempts, serious adverse events, and discontinuations because of adverse events). There were minor inconsistencies in the population in the primary efficacy analysis between the protocol and clinical study report and within the clinical study report for one trial. Furthermore, we found contradictory information within the reports for seven serious adverse events and eight adverse events that led to discontinuation but with no apparent bias. In each trial, a median of 406 (range 177-645) and 166 (100-241) treatment emergent adverse events (adverse events that emerged or worsened after study drug was started) in the randomised phase were not reported in journal articles and Lilly trial registry reports, respectively. We also found publication bias in relation to beneficial effects.
Conclusion: Clinical study reports contained extensive data on major harms that were unavailable in journal articles and in trial registry reports. There were inconsistencies between protocols and clinical study reports and within clinical study reports. Clinical study reports should be used as the data source for systematic reviews of drugs, but they should first be checked against protocols and within themselves for accuracy and consistency.
© Maund et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Digging for data on harms in duloxetine trials.BMJ. 2014 Jun 4;348:g3578. doi: 10.1136/bmj.g3578. BMJ. 2014. PMID: 24904123 No abstract available.
References
-
- Scherer RW, Langenberg P, von Elm E. Full publication of results initially presented in abstracts. Cochrane Database Syst Rev 2007;2:MR000005. - PubMed
-
- Chan AW, Hróbjartsson A, Haahr MT, Gøtzsche PC, Altman DG. Empirical evidence for the selective reporting of outcomes in randomized trials: comparison of protocols to published articles. JAMA 2004;291:2457-65. - PubMed
-
- Turner EH, Mathews AM, Linardatos E, Tell RA, Rosenthal R. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med 2008;358:252. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials