

Daily sedative interruption versus intermittent sedation in mechanically ventilated critically ill patients: a randomized trial
- PMID: 24900938
- PMCID: PMC4026117
- DOI: 10.1186/2110-5820-4-14
Daily sedative interruption versus intermittent sedation in mechanically ventilated critically ill patients: a randomized trial
Abstract
Background: Daily sedative interruption and intermittent sedation are effective in abbreviating the time on mechanical ventilation. Whether one is superior to the other has not yet been determined. Our aim was to compare daily interruption and intermittent sedation during the mechanical ventilation period in a low nurse staffing ICU.
Methods: Adult patients expected to need mechanical ventilation for more than 24 hours were randomly assigned, in a single center, either to daily interruption of continuous sedative and opioid infusion or to intermittent sedation. In both cases, our goal was to maintain a Sedation Agitation Scale (SAS) level of 3 or 4; that is patients should be calm, easily arousable or awakened with verbal stimuli or gentle shaking. Primary outcome was ventilator-free days in 28 days. Secondary outcomes were ICU and hospital mortality, incidence of delirium, nurse workload, self-extubation and psychological distress six months after ICU discharge.
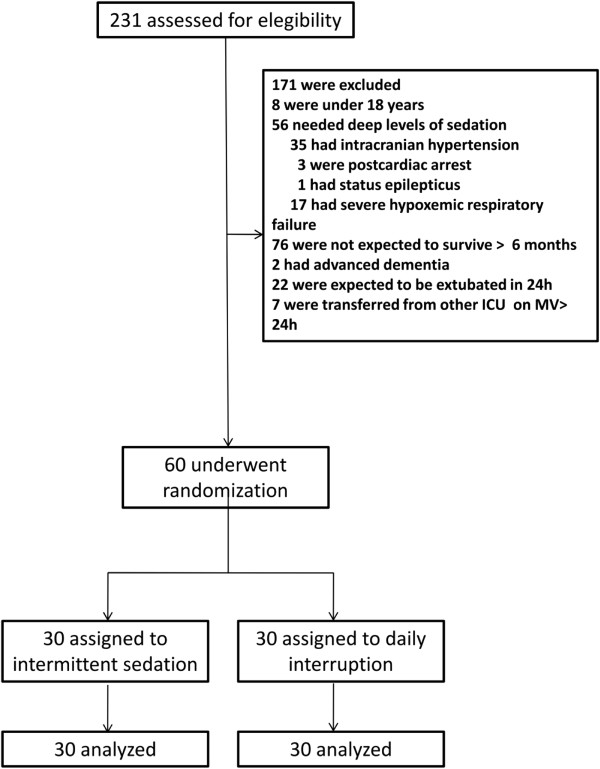
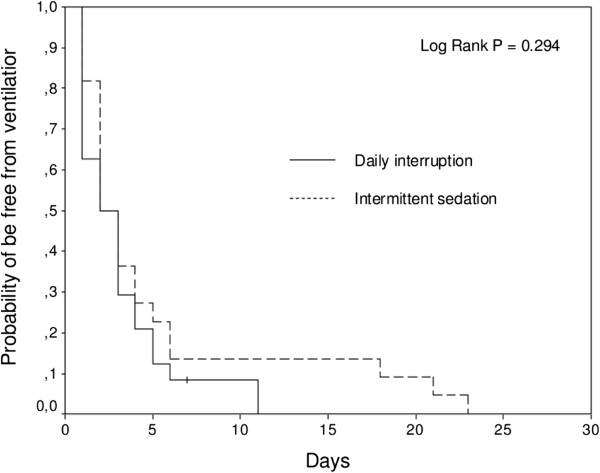
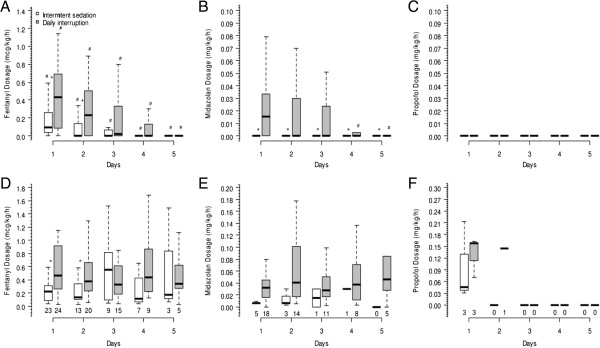
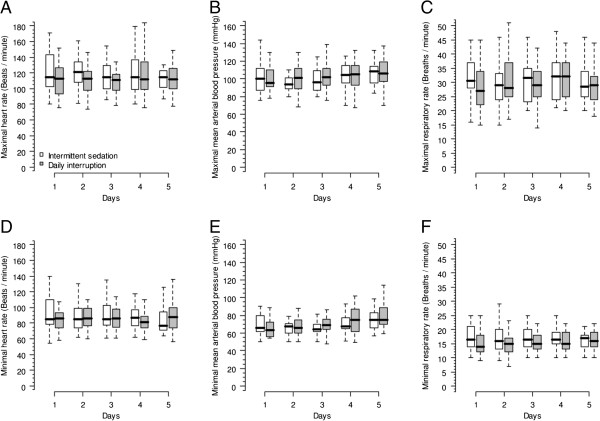
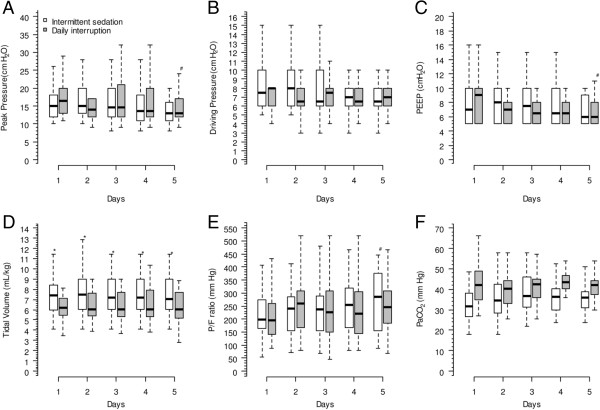
Results: A total of 60 patients were included. There were no differences in the ventilator-free days in 28 days between daily interruption and intermittent sedation (median: 24 versus 25 days, P = 0.160). There were also no differences in ICU mortality (40 versus 23.3%, P = 0.165), hospital mortality (43.3 versus 30%, P = 0.284), incidence of delirium (30 versus 40%, P = 0.472), self-extubation (3.3 versus 6.7%, P = 0.514), and psychological stress six months after ICU discharge. Also, the nurse workload was not different between groups, but it was reduced on day 5 compared to day 1 in both groups (Nurse Activity Score (NAS) in the intermittent sedation group was 54 on day 1 versus 39 on day 5, P < 0.001; NAS in daily interruption group was 53 on day 1 versus 38 on day 5, P < 0.001). Fentanyl and midazolam total dosages per patient were higher in the daily interruption group. The tidal volume was higher in the intermittent sedation group during the first five days of ICU stay.
Conclusions: There was no difference in the number of ventilator-free days in 28 days between both groups. Intermittent sedation was associated with lower sedative and opioid doses.
Trial registration: ClinicalTrials.gov Identifier: NCT00824239.
Keywords: Conscious sedation; Critical care and outcome assessment; Mechanical ventilation; Sedation.
Figures
References
-
- Salluh JI, Dal-Pizzol F, Mello PV, Friedman G, Silva E, Teles JM, Lobo SM, Bozza FA, Soares M. Delirium recognition and sedation practices in critically ill patients: a survey on the attitudes of 1015 Brazilian critical care physicians. J Crit Care. 2009;4:556–562. doi: 10.1016/j.jcrc.2009.04.004. - DOI - PubMed
-
- Shehabi Y, Bellomo R, Reade MC, Bailey M, Bass F, Howe B, McArthur C, Seppelt IM, Webb S, Weisbrodt L. Sedation Practice in Intensive Care Evaluation (SPICE) Study Investigators; ANZICS Clinical Trials Group. Early intensive care sedation predicts long-term mortality in ventilated critically ill patients. Am J Respir Crit Care Med. 2012;4:724–731. doi: 10.1164/rccm.201203-0522OC. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
