

Systemic approach to identify serum microRNAs as potential biomarkers for acute myocardial infarction
- PMID: 24900964
- PMCID: PMC4036490
- DOI: 10.1155/2014/418628
Systemic approach to identify serum microRNAs as potential biomarkers for acute myocardial infarction
Abstract
Background: Recent studies have revealed the role of microRNAs (miRNAs) in a variety of biological and pathological processes, including acute myocardial infarction (AMI). We hypothesized that ST-segment elevation myocardial infarction (STEMI) may be associated with an alteration of miRNAs and that circulating miRNAs may be used as diagnostic markers for STEMI.
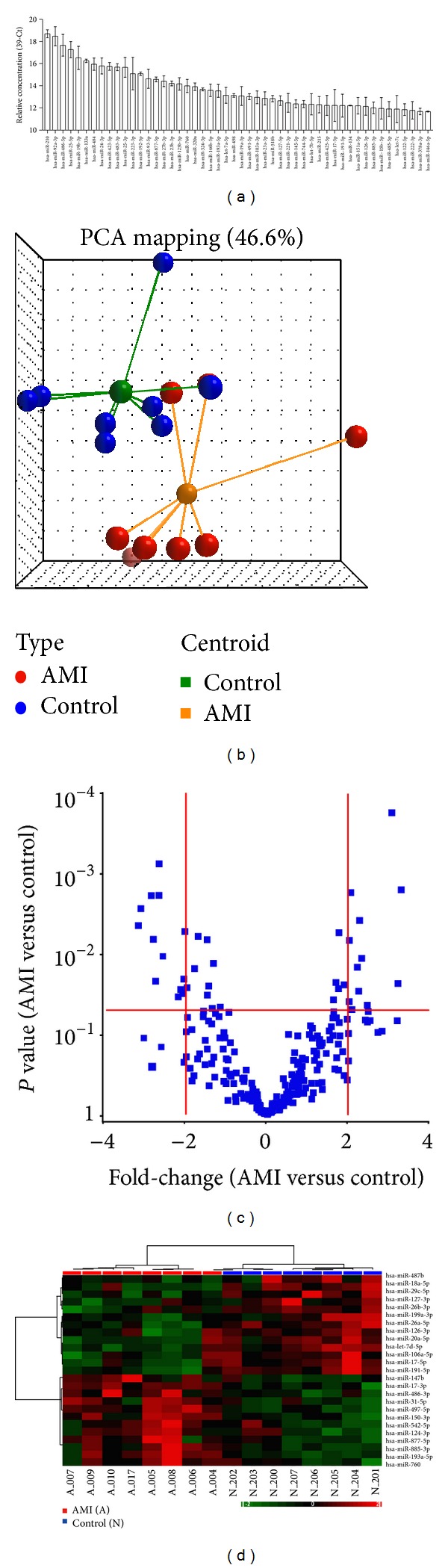
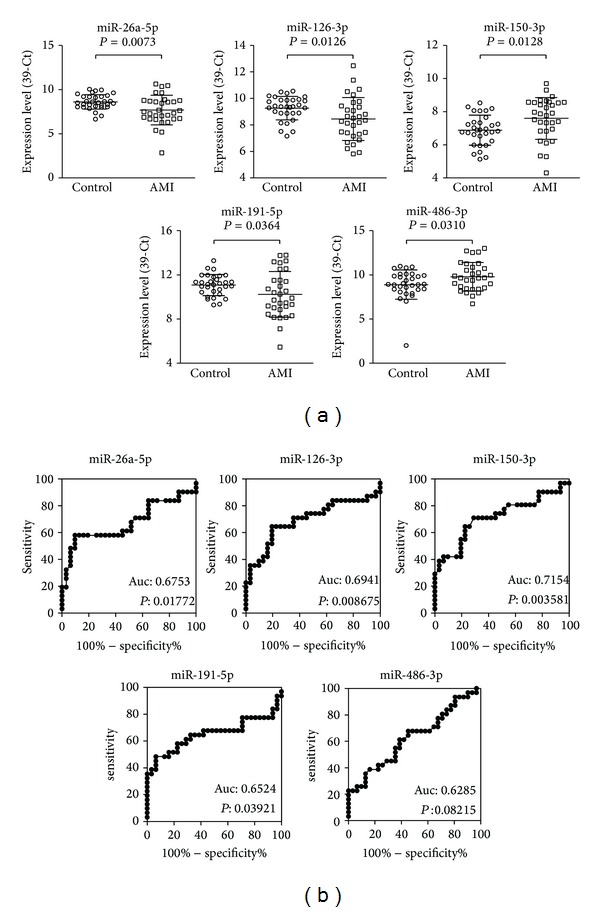
Methods: Expression levels of 270 serum miRNAs were analyzed in 8 STEMI patients and 8 matched healthy controls to identify miRNAs differentially expressed in the sera of patients with AMI. The differentially expressed miRNAs were evaluated in a separate cohort of 62 subjects, including 31 STEMI patients and 31 normal controls.
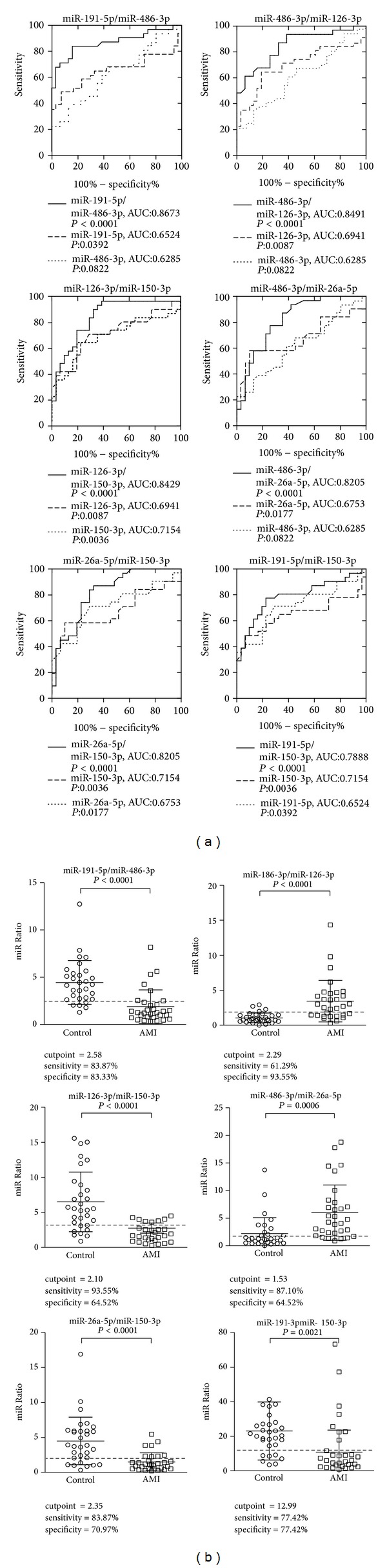
Results: The initial profiling study identified 12 upregulated and 13 downregulated serum miRNAs in the AMI samples. A subsequent validation study confirmed that serum miR-486-3p and miR-150-3p were upregulated while miR-126-3p, miR-26a-5p, and miR-191-5p were significantly downregulated in the sera of patients with AMI. Ratios between the level of upregulated and downregulated miRNAs were also significantly different in those with AMI. Receiver operator characteristics curve analysis using the expression ratio of miR-486-3p and miR-191-5p showed an area under the curve of 0.863.
Conclusion: Our results suggest that serum miRNAs may be used as potential diagnostic biomarkers for STEMI.
Figures
References
-
- O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):e362–e425. - PubMed
-
- Masoudi FA, Bonow RO, Brindis RG, et al. ACC/AHA 2008 statement on performance measurement and reperfusion therapy: a report of the ACC/AHA Task Force on Performance Measures (Work group to address the challenges of performance measurement and reperfusion therapy) Circulation. 2008;118(24):2649–2661. - PubMed
-
- Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined—a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. Journal of the American College of Cardiology. 2000;36(3):959–969. - PubMed
-
- Anderson HV, Shaw RE, Brindis RG, et al. Relationship between procedure indications and outcomes of percutaneous coronary interventions by American College of Cardiology/American Heart Association Task Force Guidelines. Circulation. 2005;112(18):2786–2791. - PubMed
-
- Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction—2002: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients with Unstable Angina) Circulation. 2002;106(14):1893–1900. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
