

Neonatal and maternal outcomes with prolonged second stage of labor
- PMID: 24901265
- PMCID: PMC4065200
- DOI: 10.1097/AOG.0000000000000278
Neonatal and maternal outcomes with prolonged second stage of labor
Erratum in
- Obstet Gynecol. 2014 Oct;124(4):842
Abstract
Objective: To assess neonatal and maternal outcomes when the second stage of labor was prolonged according to American College of Obstetricians and Gynecologists guidelines.
Methods: Electronic medical record data from a retrospective cohort (2002-2008) from 12 U.S. clinical centers (19 hospitals), including 43,810 nulliparous and 59,605 multiparous singleton deliveries at 36 weeks of gestation or greater, vertex presentation, who reached 10-cm cervical dilation were analyzed. Prolonged second stage was defined as: nulliparous women with epidural greater than 3 hours and without greater than 2 hours and multiparous women with epidural greater than 2 hours and without greater than 1 hour. Maternal and neonatal outcomes were compared and adjusted odds ratios calculated controlling for maternal race, body mass index, insurance, and region.
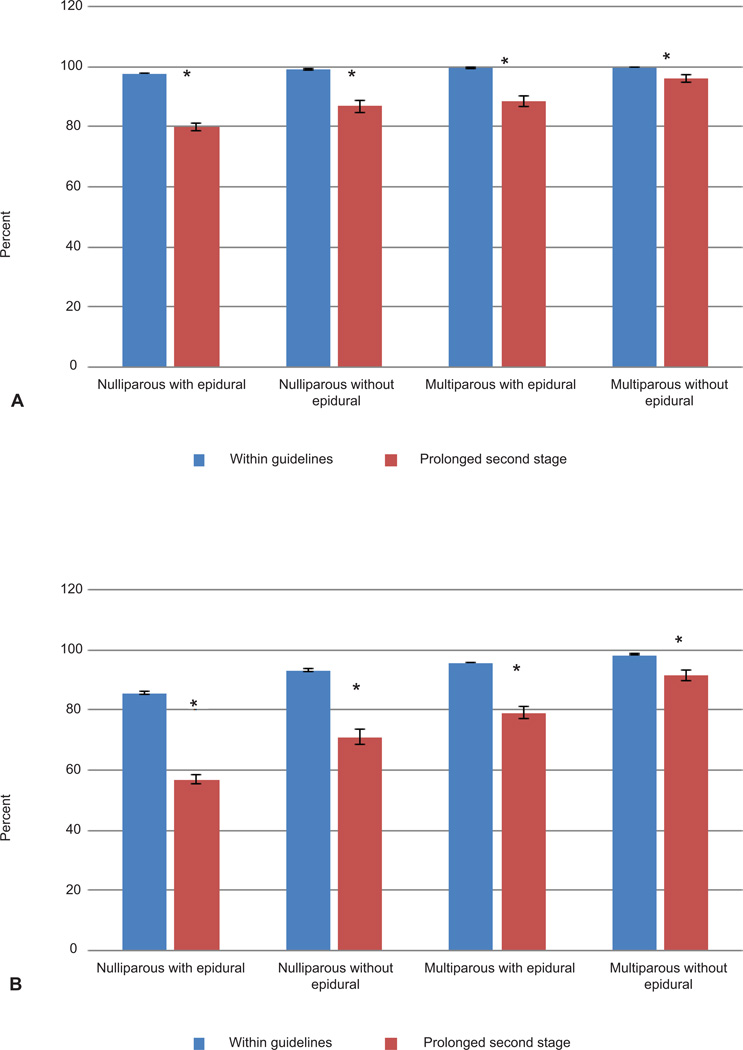
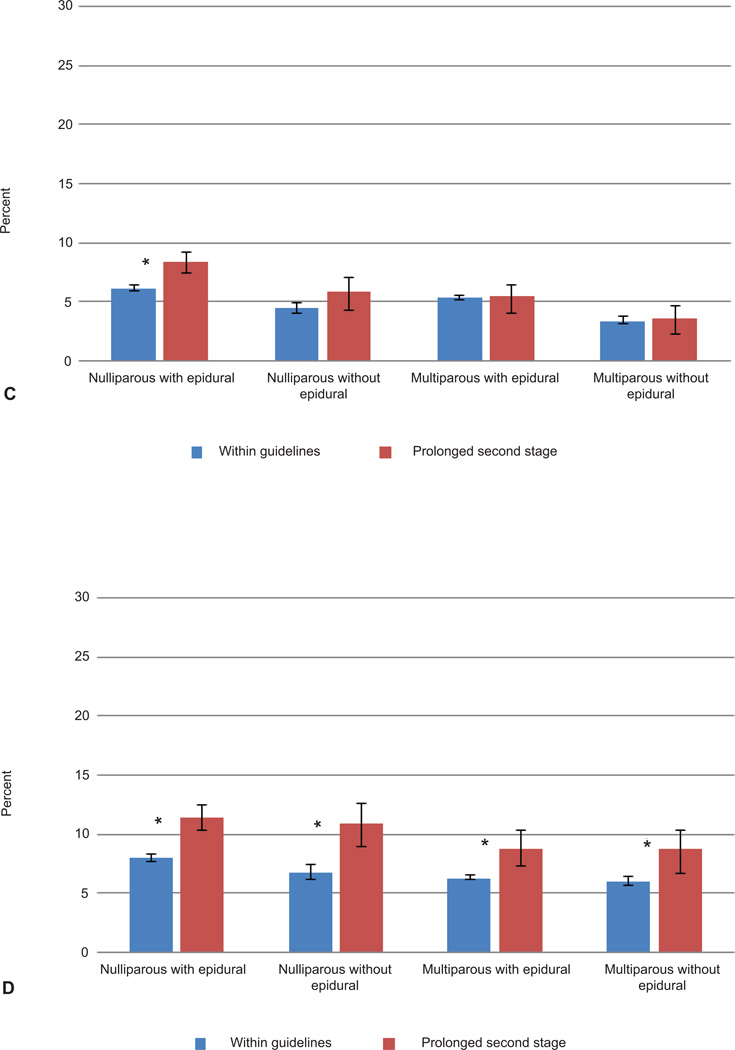
Results: Prolonged second stage occurred in 9.9% and 13.9% of nulliparous and 3.1% and 5.9% of multiparous women with and without an epidural, respectively. Vaginal delivery rates with prolonged second stage compared with within guidelines were 79.9% compared with 97.9% and 87.0% compared with 99.4% for nulliparous women with and without epidural, respectively, and 88.7% compared with 99.7% and 96.2% compared with 99.9% for multiparous women with and without epidural, respectively (P<.001 for all comparisons). Prolonged second stage was associated with increased chorioamnionitis and third-degree or fourth-degree perineal lacerations. Neonatal morbidity with prolonged second stage included sepsis in nulliparous women (with epidural: 2.6% compared with 1.2% [adjusted odds ratio (OR) 2.08, 95% confidence interval (CI) 1.60-2.70]; without epidural: 1.8% compared with 1.1% [adjusted OR 2.34, 95% CI 1.28-4.27]); asphyxia in nulliparous women with epidural (0.3% compared with 0.1% [adjusted OR 2.39, 95% CI 1.22-4.66]) and perinatal mortality without epidural (0.18% compared with 0.04% for nulliparous women [adjusted OR 5.92, 95% CI 1.43-24.51]); and 0.21% compared with 0.03% for multiparous women (adjusted OR 6.34, 95% CI 1.32-30.34). However, among the offspring of women with epidurals whose second stage was prolonged (3,533 nulliparous and 1,348 multiparous women), there were no cases of hypoxic-ischemic encephalopathy or perinatal death.
Conclusions: Benefits of increased vaginal delivery should be weighed against potential small increases in maternal and neonatal risks with prolonged second stage.
Level of evidence: : II.
Conflict of interest statement
Figures
References
-
- Hellman LM, Prystowsky H. The duration of the second stage of labor. Am J Obstet Gynecol. 1952 Jun;63(6):1223–1233. - PubMed
-
- Cohen WR. Influence of the duration of second stage labor on perinatal outcome and puerperal morbidity. Obstet Gynecol. 1977 Mar;49(3):266–269. - PubMed
-
- Moon JM, Smith CV, Rayburn WF. Perinatal outcome after a prolonged second stage of labor. J Reprod Med. 1990 Mar;35(3):229–231. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials