

Maternal prepregnancy folate intake and risk of spontaneous abortion and stillbirth
- PMID: 24901281
- PMCID: PMC4086728
- DOI: 10.1097/AOG.0000000000000343
Maternal prepregnancy folate intake and risk of spontaneous abortion and stillbirth
Abstract
Objective: To evaluate prospectively the relationship between prepregnancy folate intake and risk of spontaneous abortion and stillbirth.
Methods: Women in the Nurses' Health Study II who self-reported a pregnancy between 1992 and 2009 were included in this analysis. Dietary folate and supplement use was assessed every 4 years, starting in 1991, by a food frequency questionnaire. Pregnancies were self-reported with case pregnancies lost spontaneously (spontaneous abortion less than 20 weeks of gestation and stillbirth 20+ weeks of gestation) and comparison pregnancies ending in ectopic pregnancy, induced abortion, or live birth.
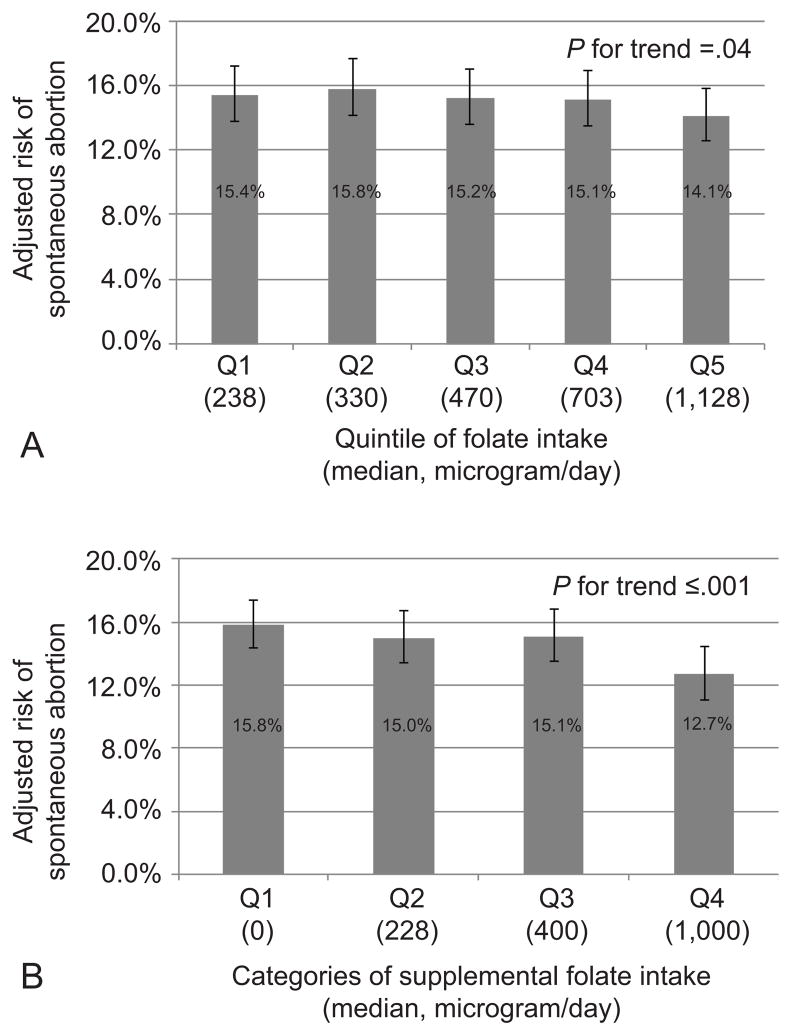
Results: Among the 11,072 women, 15,950 pregnancies were reported of which 2,756 (17.3%) ended in spontaneous abortion and 120 (0.8%) ended in stillbirth. Compared with women in the lowest quintile of prepregnancy folate intake (less than 285 micrograms/d), those in the highest quintile (greater than 851 micrograms/d) had a relative risk of spontaneous abortion of 0.91 (95% confidence interval [CI] 0.82-1.02) after multivariable adjustment (P trend=.04). This association was primarily attributable to intake of folate from supplements. Compared with women without supplemental folate intake (0 micrograms/d), those in the highest category (greater than 730 micrograms/d) had a relative risk of spontaneous abortion of 0.80 (95% CI 0.71-0.90) after multivariable adjustment (P trend <.001). The association of prepregnancy supplemental folate with risk of spontaneous abortion was consistent across gestational period of loss. A similar inverse trend was observed with the risk of stillbirth, which fell short of conventional significance (P trend=.06).
Conclusions: Higher intake of folate from supplements was associated with reduced risk of spontaneous abortion. Women at risk of pregnancy should use supplemental folate for neural tube defect prevention and because it may decrease the risk of spontaneous abortion.
Level of evidence: : II.
Figures
References
-
- Wilcox AJ, Weinberg CR, O’Connor JF, Baird DD, Schlatterer JP, Canfield RE, et al. Incidence of early loss of pregnancy. N Engl J Med. 1988;319:189–94. - PubMed
-
- Treloar AE, Boynton RE, Behn BG, Brown BW. Variation of the human menstrual cycle through reproductive life. Int J Fertil. 1967;12:77–126. - PubMed
-
- Cramer DW, Wise LA. The epidemiology of recurrent pregnancy loss. Semin Reprod Med. 2000;18:331–9. - PubMed
-
- Homan GF, Davies M, Norman R. The impact of lifestyle factors on reproductive performance in the general population and those undergoing infertility treatment: a review. Hum Reprod Update. 2007;13:209–23. - PubMed
-
- De-Regil LM, Fernandez-Gaxiola AC, Dowswell T, Pena-Rosas JP. Folic acid supplements before conception and in early pregnancy (up to 12 weeks) for the prevention of birth defects. Cochrane Database Syst Rev. 2010
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
