

Left atrial passive emptying function determined by cardiac magnetic resonance predicts atrial fibrillation recurrence after pulmonary vein isolation
- PMID: 24902586
- PMCID: PMC4219259
- DOI: 10.1161/CIRCIMAGING.113.001472
Left atrial passive emptying function determined by cardiac magnetic resonance predicts atrial fibrillation recurrence after pulmonary vein isolation
Abstract
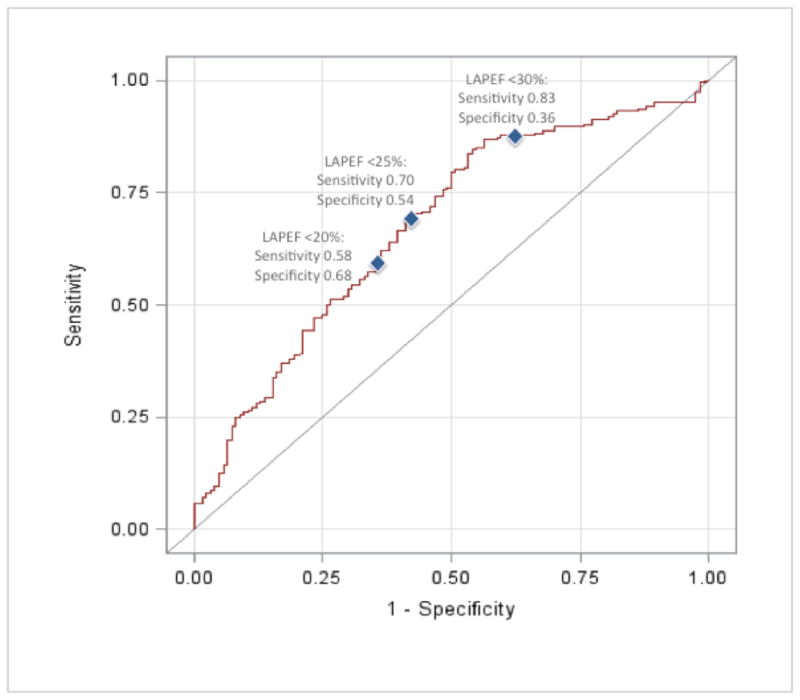
Background: Although pulmonary vein isolation has become a mainstream therapy for selected patients with atrial fibrillation (AF), late recurrent AF is common and its risk factors remain poorly defined. The purpose of our study was to test the hypothesis that reduced left atrial passive emptying function (LAPEF) as determined by cardiac magnetic resonance has a strong association with late recurrent AF after pulmonary vein isolation.
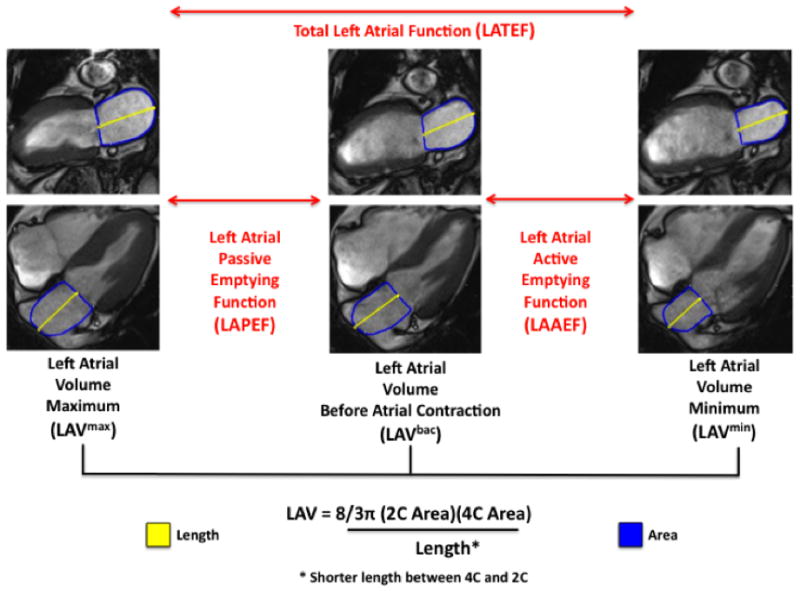
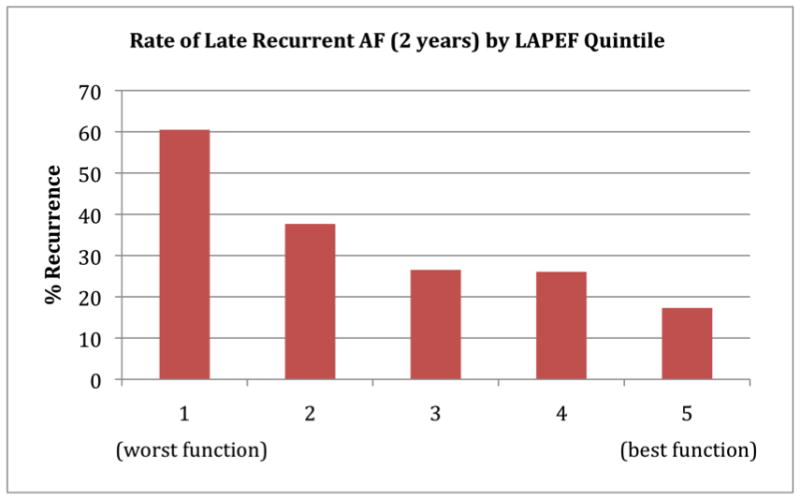
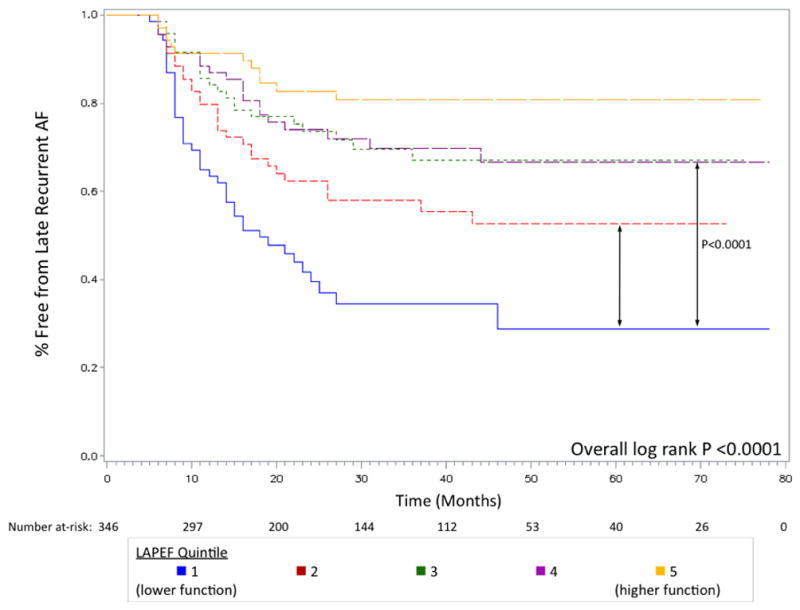
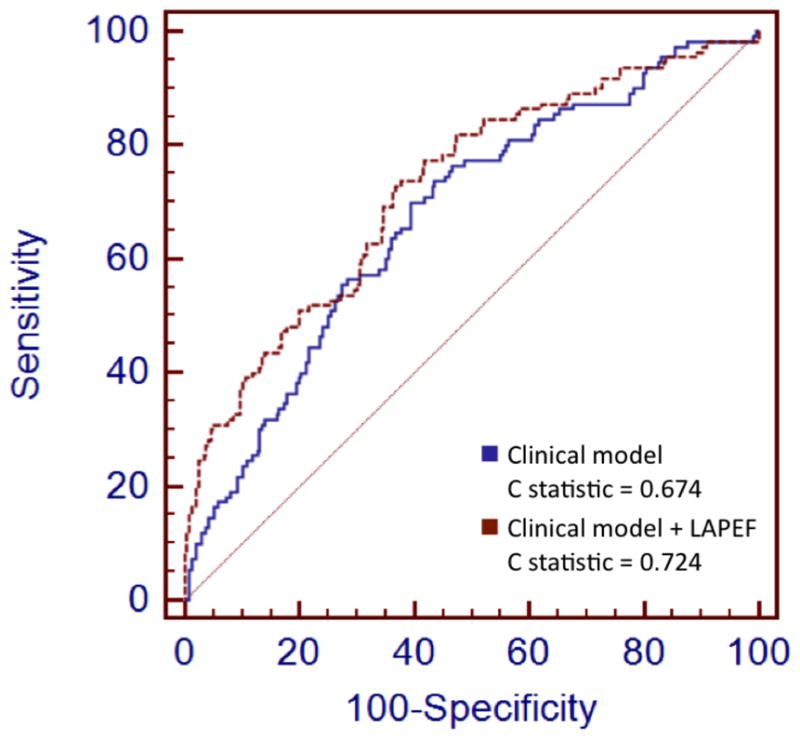
Methods and results: Three hundred forty-six patients with AF referred for cardiac magnetic resonance pulmonary vein mapping before pulmonary vein isolation were included. Maximum LA volumes (VOLmax) and volumes before atrial contraction (VOLbac) were measured; LAPEF was calculated as (VOLmax-VOLbac)/VOLmax×100. Kaplan-Meier curves were constructed to determine late recurrent AF stratified by LAPEF quintile. Cox proportional hazards regression was used to adjust for known markers of recurrence. During a median follow-up of 27 months, 124 patients (35.8%) experienced late recurrent AF. Patients with recurrence were more likely to have nonparoxysmal AF (75.8% versus 51.4%; P<0.01), higher mean VOLmax (60.2 versus 52.8 mL/m(2); P<0.01), and lower mean LAPEF (19.1% versus 26.0%; P<0.01). Patients in the lowest LAPEF quintile were at highest risk of developing recurrent AF (2-year recurrence for lowest versus highest: 60.5% versus 17.3%; P<0.01). After adjusting for known predictors of recurrence, patients with low LAPEF remained significantly more likely to recur (hazard ratio for lowest versus highest quintile, 3.92; 95% confidence interval, 2.01-7.65).
Conclusions: We found a strong association between LAPEF and recurrent AF after pulmonary vein isolation that persisted after multivariable adjustment.
Keywords: atrial fibrillation; catheter ablation; magnetic resonance imaging.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen S, Crijns HJG, Damiano RJ, Davies DW, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haines DE, Haissaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim Y, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay BD, Mansour M, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer DL, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao H, Wilber D, Calkins H, Kuck KH, Cappato R, Chen S, Prystowsky EN, Kuck KH, Natale A, Haines DE, Marchlinski FE, Calkins H, Davies DW, Lindsay BD, Damiano R, Packer DL, Brugada J, Camm AJ, Crijns HJG, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haissaguerre M, Hindricks G, Iesaka Y, Jackman WM, Jais P, Jalife J, Kalman J, Keane D, Kim Y, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Mansour M, Marchlinski F, McCarthy P, Mont JL, Morady F, Nademanee K, Nakagawa H, Nattel S, Pappone C, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao H, Wilber D, Ad N, Cummings J, Gillinov AM, Heidbuchel H, January C, Lip G, Markowitz S, Nair M, Ovsyshcher IE, Pak H, Tsuchiya T, Shah D, Siong TW, Vardas PE. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: Recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Heart Rhythm. 2012;9:632–696. - PubMed
-
- Weerasooriya R, Khairy P, Litalien J, Macle L, Hocini M, Sacher F, Lellouche N, Knecht S, Wright M, Nault I, Miyazaki S, Scavee C, Clementy J, Haissaguerre M, Jais P. Catheter ablation for atrial fibrillation: Are results maintained at 5 years of follow-up? J Am Coll Cardiol. 2011;57:160–166. - PubMed
-
- Balk EM, Garlitski AC, Alsheikh-Ali AA, Terasawa T, Chung M, Ip S. Predictors of atrial fibrillation recurrence after radiofrequency catheter ablation: A systematic review. J Cardiovasc Electrophysiol. 2010;21:1208–1216. - PubMed
-
- Berruezo A, Tamborero D, Mont L, Benito B, Tolosana JM, Sitges M, Vidal B, Arriagada G, Méndez F, Matiello M, Molina I, Brugada J. Pre-procedural predictors of atrial fibrillation recurrence after circumferential pulmonary vein ablation. Eur Heart J. 2007;28:836–841. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
