

Determination of optimal vitamin D3 dosing regimens in HIV-infected paediatric patients using a population pharmacokinetic approach
- PMID: 24902982
- PMCID: PMC4243886
- DOI: 10.1111/bcp.12433
Determination of optimal vitamin D3 dosing regimens in HIV-infected paediatric patients using a population pharmacokinetic approach
Abstract
Aims: To investigate 25-hydroxycholecalciferol [25(OH)D] population pharmacokinetics in children and adolescents, to establish factors that influence 25(OH)D pharmacokinetics and to assess different vitamin D3 dosing schemes to reach sufficient 25(OH)D concentrations (>30 ng ml(-1) ).
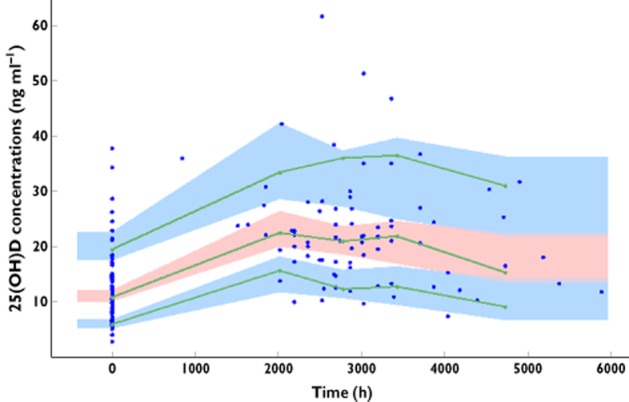
Methods: This monocentric prospective study included 91 young HIV-infected patients aged 3 to 24 years. Patients received a 100 000 IU vitamin D3 supplementation. A total of 171 25(OH)D concentrations were used to perform a population pharmacokinetic analysis.
Results: At baseline 28% of patients had 25(OH)D concentrations below 10 ng ml(-1) , 69% between 10 and 30 ng ml(-1) and 3% above 30 ng ml(-1) . 25(OH)D pharmacokinetics were best described by a one compartment model with an additional production parameter reflecting the input from diet and sun exposure. The effects of skin phototype and bodyweight were significant on 25(OH)D production before any supplementation. The basal level was 27% lower in non-white skin phototype patients and was slightly decreased with bodyweight. No significant differences in 25(OH)D concentrations were related to antiretroviral drugs. To obtain concentrations between 30 and 80 ng ml(-1) , patients with baseline concentrations between 10 and 30 ng ml(-1) should receive 100 000 IU per 3 months. However, vitamin D deficient patients (<10 ng ml(-1) ) would need an intensive phase of 100 000 IU per 2 weeks (two times) followed 2 weeks later by a maintenance phase of 100 000 IU per 3 months.
Conclusions: Skin phototype and bodyweight had an influence on the basal production of 25(OH)D. According to 25(OH)D baseline concentrations, dosing schemes to reach sufficient concentrations are proposed.
Keywords: 25-hydroxycholecalciferol; HIV-infected patients; children and adolescents; population pharmacokinetics.
© 2014 The British Pharmacological Society.
Figures
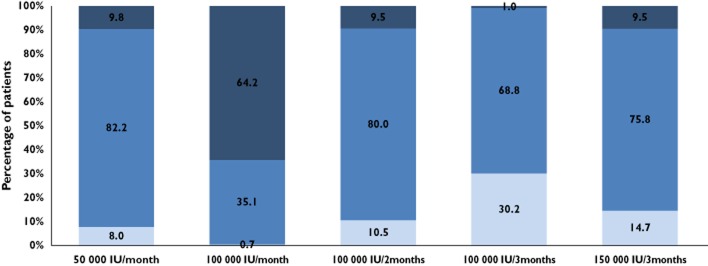
 , <30 ng ml−1;
, <30 ng ml−1;  , 30–80 ng ml−1;
, 30–80 ng ml−1;  , >80 ng ml−1
, >80 ng ml−1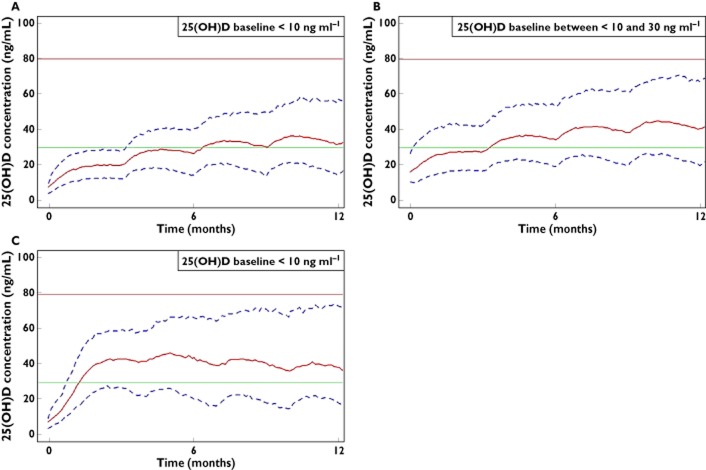
References
-
- Dao CN, Patel P, Overton ET, Rhame F, Pals SL, Johnson C, Bush T, Brooks JT. Low vitamin D among HIV-infected adults: prevalence of and risk factors for low vitamin D Levels in a cohort of HIV-infected adults and comparison to prevalence among adults in the US general population. Clin Infect Dis Off Publ Infect Dis Soc Am. 2011;52:396–405. - PubMed
-
- Kim JH, Gandhi V, Psevdos G, Espinoza F, Park J, Sharp V. Evaluation of vitamin D levels among HIV-infected patients in New York City. 2011. AIDS Res Hum Retroviruses [Internet]. Available at http://www.ncbi.nlm.nih.gov/pubmed/21644847 (last accessed 27 November 2011) - PubMed
-
- Mueller NJ, Fux CA, Ledergerber B, Elzi L, Schmid P, Dang T, Magenta L, Calmy A, Vergopoulos A, Bischoff-Ferrari HA. High prevalence of severe vitamin D deficiency in combined antiretroviral therapy-naive and successfully treated Swiss HIV patients. AIDS Lond Engl. 2010;24:1127–1134. - PubMed
-
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–281. - PubMed
-
- Vieth R, Bischoff-Ferrari H, Boucher BJ, Dawson-Hughes B, Garland CF, Heaney RP, Holick MF, Hollis BW, Lamberg-Allardt C, McGrath JJ, Norman AW, Scragg R, Whiting SJ, Willett WC, Zittermann A. The urgent need to recommend an intake of vitamin D that is effective. Am J Clin Nutr. 2007;85:649–650. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
